Quadratus Lumborum Block: A More Extensive Spread and Longer-Lasting Alternative to the Tranversus Abdominus Plane Block?
By Franklin Chiao, MD and Boyoun Jung, MD
New York Presbyterian Medical Center-Weill Cornell Medicine
The quadratus lumborum block (QLB) is a relatively underutilized trunk block that can be considered a regional anesthesia option for truncal surgery along with epidural, paravertebral (PVB), and transversus abdominus plane (TAP) blocks1. The literature can be confusing as it has also been called a “posterior TAP” block in several papers and several different injection sites have been studied. Local anesthetic is injected into the fascial plane next to the quadratus lumborum muscle (Figure 1) and can potentially spread to the thoracic paravertebral space as seen with MRI contrast2.
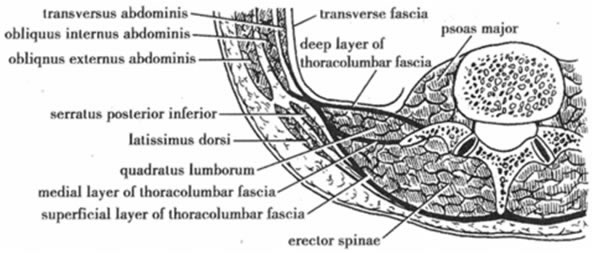
Figure 1: QLB Anatomy3
It has several advantages versus the TAP block. QLB is a wider and longer-lasting block compared to a TAP block, spreading between T7 to T12/L1 with a single injection compared to smaller coverage with a TAP block- sometimes only 3 dermatomes-(Figure 2)1,4. With the same total dose of ropivacaine, the analgesic effect was shown to last more than TAP (21 hours for QLB vs 7 hours for TAP)-(Figure 3)4. Peak arterial ropivacaine concentrations were also significantly lower in QLB than TAP block; however the study used 0.375% ropivacaine for QLB and 0.5% for TAP (Figure 3).
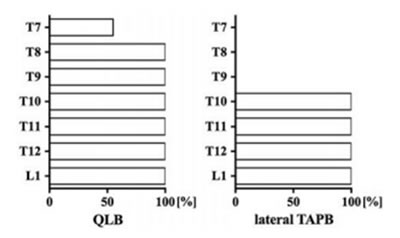
Figure 2 - Dermatomal effects of QLB versus lateral TAP. X-Axis is sensory coverage success rate4
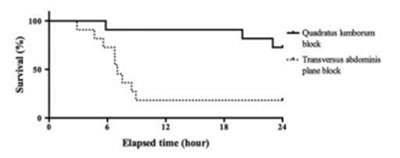
Figure 3 - Kaplan Meier survival curve of time from block to first post-operative analgesic rescue4
PVB is a regional anesthetic option for truncal surgery and may have comparable duration as QLB, but is associated with risks of hypotension and vascular puncture, as well as iatrogenic pneumothorax1,4. It is technically challenging and considered by some to be an advanced regional anesthetic technique. Epidural block is associated with a greater degree of hypotension than QLB and risks thereof include intrathecal injection, infection, and epidural hematoma.
QLB is still a relatively new technique, so it is possible that limitations will be discovered in further prospective clinical research. Some questions include: Which position is optimal for image and needle guidance? What is the failure/complication rate? When it spreads to paravertebral space, where is the evidence of hypotension? How reliable is the long duration?
QLB can be performed supine, but is more easily placed when the patient has a hip raised or is in the lateral decubitus position. A high frequency linear US transducer may be used as the structures are not as deep as in adults in whom a lower frequency probe may be necessary. The probe is placed on the flank in Petit’s triangle (iliac crest inferiorly, latissimus dorsi posteriorly, and external oblique anteriorly) (Figure 4) and as the transducer is moved dorsally, external oblique and internal oblique disappear into an aponeurosis as latissimus dorsi appears. The quadratus lumborum muscle appears beneath latissimus dorsi (Figure 5). Several needle approaches and injection sites have garnered attention. In an MRI contrast study, it appears the transmuscular needle approach has more reliable spread of local into the paraverterbral space (Figure 6)5. Transmuscular injection of local occurs between quadratus lumborum and psoas major muscle is demonstrated in figure 6 and this is known as a type 3 quadratus lumborum block. Blanco originally labelled some anterior injection locations as type 1 and type 2 (Figure 7), but has since referred to type 2 as the “QLB” because of the greater analgesia with the more posterior type 2 approach6. Dosing in adults has been shown to be less than that required for a TAP block. In pediatrics, different doses have been used and are described below.
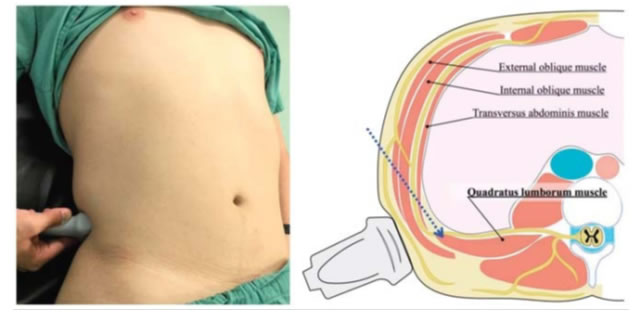
Figure 4 - QLB positioning with probe4
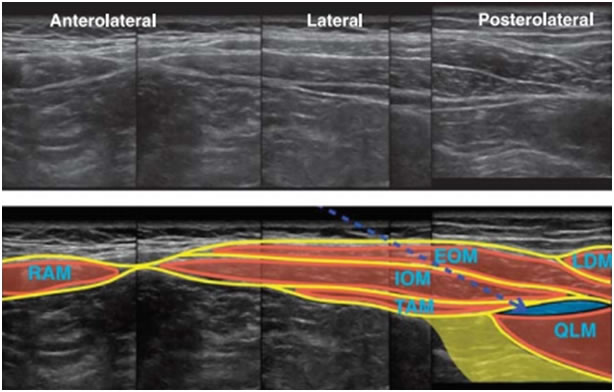
Figure 5 - Ultrasound images of QLB4
RAM: rectus abdominus muscle; EOM: external oblique muscle; IOM: internal oblique muscle; LDM: latissimus dorsi muscle; QLM: quadratus lumborum muscle
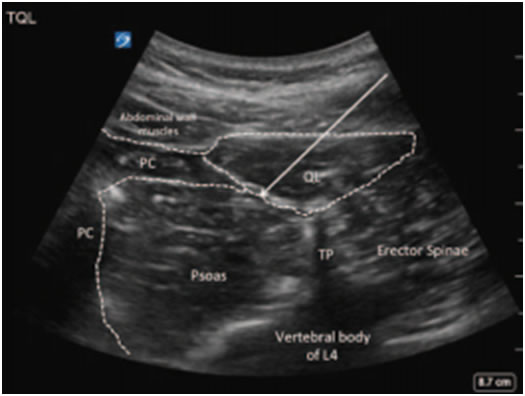
Figure 6 - Transmuscular needle approach to QLB-image modified5
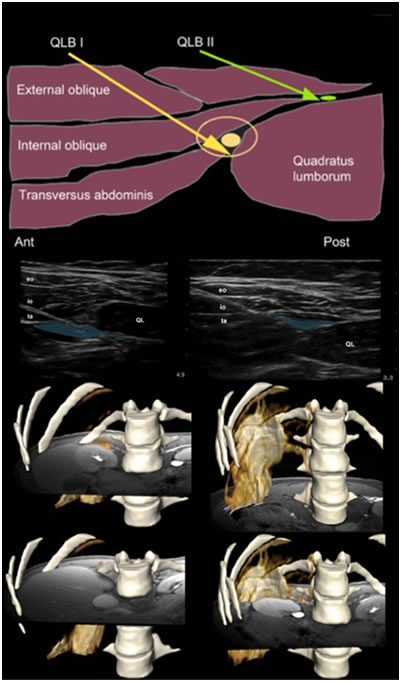
Figure 7 - Quadratus Lumborum Type 1 and 2 as elucidated by Blanco8 in a contrast injection.
Several case reports of successful use of a QLB catheter in pediatrics have been reported for prolonged post-operative analgesia with bolus doses varying between 0.25-0.5ml/kg and infusions running at 5ml/hr or about 0.25ml/kg/hr.
A 7 year old girl undergoing radical nephrectomy for resection of a Wilms tumor required no additional analgesic other than paracetamol throughout the first 4 days while she had the catheter infusing levobupivacaine 0.1% 1. A 5 year old girl undergoing colostomy for blunt rectal trauma required minimal analgesic with a catheter infusion of ropivacaine 0.2% 7.
The QLB is gaining in popularity as an analgesic option for truncal surgery in both pediatrics and adults. There is a growing body of literature highlighting its effectiveness. With additional clinical research, the limitations, optimal approach and dosing should become better delineated.
Please take a brief QLB Survey - https://www.surveymonkey.com/r/ZJ76Y36
References
- Chakraborty A, Goswami J, Patro V. Ultrasound-guided continuous quadratus lumborum block for postoperative analgesia in a pediatric patient. A A case reports. 2015;4(3):34-36. doi:10.1213/XAA.0000000000000090.
- Børglum J, Jensen K, Moriggl B, et al. Ultrasound-Guided Transmuscular Quadratus Lumborum Blockade. BJA Out Blue e-Letters. 2013;(March). http://bja.oxfordjournals.org/forum/topic/brjana_el%3B9919.
- Kadam VR. Ultrasound-guided quadratus lumborum block as a postoperative analgesic technique for laparotomy. J Anaesthesiol Clin Pharmacol. 2013;29(4):550-552. doi:10.4103/0970-9185.119148.
- Murouchi T, Iwasaki S, Yamakage M. Quadratus Lumborum Block: Analgesic Effects and Chronological Ropivacaine Concentrations After Laparoscopic Surgery. Reg Anesth Pain Med. 2016;41(2):146-150. doi:10.1097/AAP.0000000000000349.
- Hansen CK, Dam M, Bendtsen TF, Børglum J. Ultrasound-Guided Quadratus Lumborum Blocks. A A Case Reports. 2016;6(2):39. doi:10.1213/XAA.0000000000000270.
- Blanco R, Ansari T, Girgis E. Quadratus lumborum block for postoperative pain after caesarean section: A randomised controlled trial. Eur J Anaesthesiol. 2015;32:812-818. doi:10.1097/EJA.0000000000000299.
- Visoiu M, Yakovleva N. Continuous postoperative analgesia via quadratus lumborum block - An alternative to transversus abdominis plane block. Paediatr Anaesth. 2013;23(10):959-961. doi:10.1111/pan.12240.
- Blanco R, McDonnell JG. Optimal point of injection: The quadratus lumborum type I and II blocks. http://www.respond2articles.com/ANA/forums/post/1550.aspx. Published 2013.
![]()