

Preoperative Pregnancy Testing: To Test or Not to Test? (An Anesthesiologist’s Dilemma)
 By H. Mayumi Homi, MD
By H. Mayumi Homi, MD
Duke University Medical Center
and Zulfiqar Ahmed, MBBS FAAP
Children's Hospital of Michigan, Detroit
In the world of pediatric anesthesia, the size, shape, and ages of our patients change quickly from case to case. Among the many challenges of managing the pediatric patient population, the adolescent group requires a unique approach especially when the topic of preoperative pregnancy testing comes up.
Preoperative pregnancy testing has been a controversial subject in anesthesiology for many years. This has been among the most variable practices all across the country as well as across the continents. Many anesthesia departments mandate preoperative pregnancy testing before surgery on all patients of reproductive age while others rely on the preoperative assessment to determine the need for pregnancy testing. Much of the data at present is subjective and actually justifies the opinion of the beholder.
The following article will review the ongoing discussions that have occurred in the literature, and present the many questions that have arisen from these articles, such as:
- Is routine preoperative pregnancy testing in adolescents justified?
- Has the literature established any guidelines?
- Who and when should be tested?
- Is it a cost-effective practice?
- If tested and the result is positive, what then?
One important piece to help address these questions has been provided by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation (Practice Advisory for Pre-Anesthesia Evaluation. Anesthesiology 96:485-496, 2002). This Task Force published its advisory in 2002 following the ASA House of Delegates meeting October 2001. At that time, the House of Delegates reviewed 5 studies that were related to preoperative pregnancy tests where routine pregnancy tests uncovered positive findings in 0.3-2.2% of cases.
The results of testing led to changes in clinical management with delays or cancellation of surgery in 100% of the cases with positive pregnancy results. The Task Force also recognized at this time that a history and physical examination may be insufficient for identification of early pregnancy. According to the task force, pregnancy testing may be considered for all female patients of childbearing age. Clinical characteristics to consider include an uncertain pregnancy history or a history suggestive of current pregnancy.
One of the articles that contributed to the advisory in 2002 was the early work by Manely et al from Chicago regarding pregnancy testing in the ambulatory setting (Preoperative Pregnancy Testing in Ambulatory Surgery: Incidence and Impact of Positive Results. Anesthesiology vol 83 (4), October 1995, 690-693). Among 2,056 women of childbearing potential who presented for ambulatory surgery, testing revealed 7 pregnancies which were previously unrecognized, for an incidence of 0.3%. Pregnancy tests were routinely performed preoperatively within 6 days of the scheduled surgery.
Occasionally, when tests were not previously performed, urine or blood for hCG (human chorionic gonadotropin) were obtained on the day of surgery in the ambulatory surgery unit. The authors concluded that the incidence of previously unrecognized pregnancy in menstruating women presenting for ambulatory, nonobstetric surgery was 0.3%. The knowledge of a positive pregnancy test resulted in cancellation or postponement of the operative procedure, with patient desire for cancellation as the main determining factor in each case.
Another article considered for the advisory came from Azzam et al from St Louis who presented a two-year retrospective chart review on the incidence of positive pregnancy testing in 412 adolescent females (Preoperative pregnancy testing in adolescents. Anesth Analg 1996; 82: 4-7). The overall incidence of positive pregnancy results in their study was 1.2%. However, in this study the patients were divided in 2 groups (under 15 years of age and 15 years and older), and there was an incidence of 2.4% of positive tests in the 15 years and older group, but no positive test results in the younger age group less than 15 years of age.
The authors concluded that mandatory pregnancy testing is advisable in adolescent surgical patients aged 15 years and older. This paper generated an impassioned debate via letters to the editor. Of the many letters, two are as follows:
- Anesth Analg 1996; 83, 438: Twersky et al argue that although the teratogenic and abortive effects on the human fetus of the more commonly used anesthetics appear at this time to be equivocal, the medico-legal implications of performing anesthesia and surgery in a pregnant patient continue to justify establishing the elective patient’s pregnancy status.
- Anesth Analg 1996; 83, 439: Kettler addresses in this letter the cost of detecting one positive pregnancy and presents a different argument. According to the author, if the charge per patient for one pregnancy test is $25, the cost of detecting one pregnancy when testing all is about $7,750.00. The author concludes that “Considering the lack of consensus as to what to do with this information we need to question whether this is a cost- effective procedure”.
A year after the 2002 advisory from the Task Force, and while the debate and confusion continued in the literature, ASA members on the Committee on Ethics and Committee on Practice Parameters published an article in the ASA Newsletter in 2003 (ASA Newsletter October 2003, Vol 67, N 10). In the article, the Committee declared that:
State of pregnancy is very personal information that belongs to the patient, and it does not alter her right to proceed with anesthesia and surgery if she so desires. Therefore, pregnancy testing should be offered to patients but should not be required by physicians unless there is a compelling medical reason to know whether the patient is pregnant. Beyond not being ethical, it also may not be legal to test a patient for pregnancy without her consent. Minors are even more complex in this regard because states have disparate statutes defining whether parents are entitled to the results of their minor child’s pregnancy testing.
Three years later in another ASA Newsletter article, the Associate Director of Professional Affairs for the ASA presented discussions from a listserve on how and when to test, whom to test, and whether a separate consent should be necessary (Bierstein K. Preoperative pregnancy testing: mandatory or elective. ASA Newsletter. July 2006, Vol 70 No 7). This article suggested that there was consensus amongst most practices that pregnancy testing is needed in some patients who deny possibility of being pregnant and that obtaining a urine HCG sample on the day of surgery is the method of choice when serum HCG testing is not available prior to the procedure. The choice of whom to test varied greatly among institutions.
Although the newsletter article was not specific to minors, an example was given where a father sued an institution when his daughter had been pregnancy tested without his consent. This case resulted in a change in the hospital’s testing policy by requiring a questionnaire to help determine the pregnancy risk category prior to testing. Informing the patient or family of the risks of refusing pregnancy testing for elective surgery and anesthesia is advised, as is documentation of refusal, and perhaps even signature of waiver releasing providers from liability.
In response to this, in November 2006, the ASA Committee on Ethics weighed in again on the topic (Ethical Dilemma of Blanket Unconsented Pregnancy Tests. ASA Newsletter. November 2006, Vol 70 No 11). The following statement was made: I was distressed to read the July 2006 “Practice Management” column “Preoperative Pregnancy Testing: Mandatory or Elective?” concerning preanesthesia pregnancy testing. In interpreting some of the legal issues, scant attention was given to the ethical/privacy/minor patient concerns, which we discussed in detail by a 2003 Joint Task Force on pregnancy testing (members of the practice parameter group on preanesthesia testing and the Committee on Ethics who were jointly appointed by the ASA president).
The ASA Committee on Ethics, the ASA Joint Task Force on Pregnancy Testing and the revised Preanesthesia Evaluation practice advisory all agree that unconsented pregnancy testing is unethical in most situations involving competent patients. The revised practice parameter advises that pregnancy testing should be “offered” to women patients. If medically indicated, it should be specifically consented to, and the patient should indicate whom, other than herself, she would want to know her results (spouse, common law partner, parents, her insurance companies, her employer?).
Clearly there remained issues of clarity in the discussions and statements. To put some objectivity in the argument, and to again address the cost, Kahn et al published a paper in 2008 in A&A discussing the incidence and the cost factor in pregnancy testing (One year experience with day-of-surgery pregnancy testing before elective orthopedic procedures. Anesth Analg 2008; 106 (4): 1127-31).
According to the authors, the ambulatory center implemented a policy of testing for urine hCG in all women of childbearing age on the day of surgery. A retrospective chart review shoed that out of 2,588 women of childbearing age who were tested the authors found five positive tests in which three were previously unrecognized pregnancies, one unrecognized ectopic pregnancy, and one was a false-positive result in a premenopausal woman. The authors concluded that “A policy of routinely performing urine hCG pregnancy tests in women of childbearing age on the day of surgery was effective in detecting unrecognized pregnancy. This resulted in a postponement of elective surgery in all cases. Of 2,588 women tested, one had surgery postponed because of a false-positive result. The cost of $3273 per true positive test must be compared with the benefit.”
In response to the article on cost effectiveness, a letter was published in May 2009 (Anesth Analg May 2009; Vol 108, No 5) that reminded practitioners that routine pregnancy testing before elective anesthesia is not an American Society of Anesthesiologists standard. The Task Force recognizes that patients may present for anesthesia with early, undetected pregnancy, and they believe that the literature is inadequate to inform patients or physicians on whether anesthesia causes harmful effects on early pregnancy. Therefore, the suggestion remained that pregnancy testing may be offered to female patients of childbearing age and for whom the result would alter the patient’s management.
The ASA-approved amended advisory, which is based on a thorough literature review, does not require pregnancy testing, and it can defend anesthesiologists who offer, but do not require or routinely order pregnancy testing. Additionally, the ASA Committee on Ethics stated that pregnancy testing should be offered and that informed consent be obtained from competent patients.
A nice guideline for testing has been outlined in the book “Evidence Based Anesthesia Practice” by Lee A. Fleisher.
Recommendations for preoperative pregnancy testing
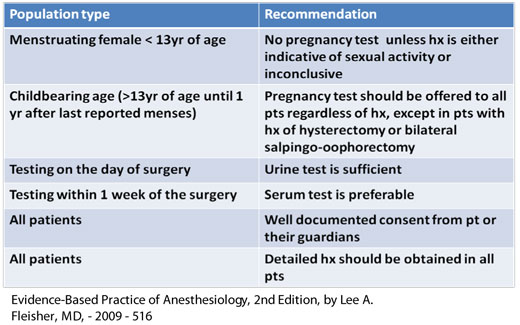
Although it seems that there are some established recommendations published in textbooks such as the one above by Dr. Fleisher, the need for a pregnancy testing for all women at childbearing age remains controversial. Even more complex is that the approach for these patients varies, specifically related to the adolescent group. It is variable among institutions and anesthesiologists based on their clinical practice, institutional polices, state laws, ethical issues, and beliefs. Most likely each individual institution needs to revise their own polices and adapt them accordingly for the adolescent patient.
Part of these considerations needs to take into account what constitutes a questionable history, whether to interview the adolescent in the presence of the parent or alone, what to do with the results if positive, and what is the lower age of testing (13 or 15?). It is important to remember that a minor, when pregnant, is only emancipated when it comes to decisions regarding pregnancy, not full emancipation. A minor can become emancipated if she meets other criteria (getting married, for example), but pregnancy itself does not emancipate a minor. This makes the decision process regarding testing and results very complicated, and a practice needs to have clear guidelines as to who will deliver the news, and who receives the news, regarding pregnancy testing results.
In conclusion, and based on review of available literature, the following may be stated:
- Routine preoperative pregnancy testing for all female of childbearing age remains controversial.
- To date, and according to the majority of the literature with the exception of the ASA newsletter article from July 2006 stating it to be mandatory, pregnancy testing is optional.
- One important point agreed upon so far is that “Pregnancy testing should be considered for all females of childbearing age”.
- Per Ethics Committee, pregnancy testing should be offered and informed consent should be obtained from competent patients and/or parents.
- Patients who receive pregnancy testing without knowledge or consent in an effort to “protect” anesthesiologists from future legal claims are not ethically, scientifically or legally supportable.
- When performed, urine hCG seems to be the test of choice on the day of surgery.
For the pediatric practitioner, it is a subject of further complexity due to the nature of taking care of adolescents and the varying levels of physical and emotional maturity as well as the legal aspects of guardianship. There is much work to do in this area for the adolescent patient and the best that is offered at this point is from adult literature. Each practice should take the guidelines offered and adapt them to what is needed in their own environment, but keeping the very basic principles intact, and the nuances of the adolescent female in mind.
![]()