



SPA Offers Many Opportunities
The spring SPA meeting is here even as the great memories of IAPA remain. I hope this newsletter serves to remind everyone of the great accomplishments (and opportunities) from IAPA as well as presenting a foretaste of the upcoming spring meeting in Vegas.
Advanced second year fellowships are increasingly popular within our specialty. Look for an important announcement on this topic within the newsletter. In addition, we present a number of review articles with an endocrine flavor (diabetes, pheochromocytoma). Returning after a period of absence is a pro/con debate. This one addresses the topic of compartment syndrome and regional anesthesia. Journal Review makes a welcome return and I look forward to this being a regular part of the newsletter. For this edition, we review recent articles from the British Journal of Anesthesia.
SPA members are often “in the news”. See who has been quoted or highlighted in the broader media recently. Please do send me announcements like the one in this newsletter so that we may celebrate the diverse accomplishments of our fellow members.
I’d like to encourage members to take the opportunity presented by the spring meeting to join one of the many working committees of SPA. There is undoubtedly one that matches the interests and skills of every member. They are a fabulous way to meet colleagues, establish contacts, make new friends and contribute to the ongoing and sustained success of our wonderful society.
Thanks in advance! Enjoy SPA 2013 at the Red Rock Casino, Resort and Spa in Las Vegas and have a wonderful year.
Please take a few minutes to read the IAPA scholars reports included in this newsletter… you’ll be glad you did. They provide a wonderful insight to the working conditions of the scholars and the impact IAPA had, and continues, to have on them.
![]()
NEW! Second Year Advanced Pediatric Anesthesia Fellowship Network
Dean Andropoulos, MD
Texas Children’s Hospital
Scott Walker, MD
Riley Children’s Hospital
Co-Chairs, PALC/PAPD Task Force on Second Year Pediatric Anesthesia Fellowships
February 5, 2013
The Pediatric Anesthesia Leadership Council (PALC) and the Pediatric Anesthesia Program Directors Association (PAPDA) are pleased to announce the organization of a network for sponsoring second year advanced pediatric anesthesia fellowships. This network was finalized at the November 1, 2012 PALC/PAPD joint meeting. These fellowships are optional 12-month fellowships after the successful completion of an ACGME accredited Pediatric Anesthesia Fellowship. The PALC and PAPDA have organized this network in response to the need to better train and equip pediatric anesthesiologists for academic and leadership roles, and for the challenges of the modern job market. The advanced fellowships are:
- Cardiac
- Research
- Pain
- Education
- Quality and Outcomes Leadership
More details about each program that offers these fellowships are now posted on the SPA website's “Pediatric Anesthesia Fellowships” page, at http://www.pedsanesthesia.org/advfellowships.iphtml. Fellowships offered and program director contact information, as well as salary and other information are contained in the “Second Year Advanced Fellowship Master Spreadsheet”, which is an Excel workbook; the first spreadsheet is an overview of all programs offering the second year fellowships; behind it is a separate spreadsheet for each program with more details. A tab at the bottom of the workbook identifies each program. A common Second Year Advanced Fellowship Application form is also included on the page.
Of the 46 ACGME accredited Pediatric Anesthesia fellowship programs, 21 offer at least one of these advanced fellowships. Eighteen offer the Cardiac Anesthesia fellowship, 17 offer the Research fellowship, nine the Pain fellowship, 4 the Education fellowship, and six the Quality and Outcomes Leadership fellowship. There are a total of 68 positions available. Current first year pediatric anesthesia fellows are encouraged to apply for the July 1, 2013 start of the PALC/PAPDA network fellowships program.
Although many institutions have offered advanced fellowships for a number of years, this effort is the first to organize them on the national level. Subcommittees in each of the fellowship areas have drafted detailed Program Requirements and curriculum documents to serve as a guide for these new programs. These programs are all certified by the local Graduate Medical Education authority when possible, and offer a Diploma or Certificate upon successful completion. In addition, several of these fellowships also offer an advanced degree such as a Master’s Degree, or a Certificate of special competency.
Salary varies by institution but is at least at the PGY-6 level; a number of positions offer increased salary above PGY-6 with part time work as an attending anesthesiologist. National Institutes of Health Loan Repayment Program of up to $35,000 per year can also be applied for with the Research Fellowships.
Applicants from outside first year fellowship programs are welcomed for most of these fellowships. Application deadlines vary but fellows are encouraged to apply as soon as possible. Further information with detail about each individual fellowship is contained in the Fellowship Listings.
Further questions can be directed to: Dean Andropoulos, M.D.; dra@bcm.edu; or Scott Walker, M.D.,; swalker1@iupui.edu.
Frequently Asked Questions about the Advanced Second Year Pediatric Anesthesia Fellowships
I already have five years of training after medical school. Why would I want to do one of these second year fellowships?
The first year fellowship is by necessity a clinical fellowship covering the range of pediatric anesthesia practice. Modern clinical and non-clinical information and roles have expanded dramatically, and there is a need for some pediatric anesthesiologists to have specialized training to adequately prepare them for leadership roles in both academic and non-academic departments.
Is this second year of training required? Is it ACGME accredited?
The second year fellowship is optional; there is one of these advanced fellowships available for every three first year fellows. The second year fellowships are not ACGME accredited, with the exception of several of the Pain fellowships.
Do all 46 ACGME Pediatric Anesthesiology Fellowships offer the advanced second year fellowships?
No; 21 of the 46 ACGME programs will also offer at least one advanced second year fellowship.
When is the application deadline for these fellowships?
Deadlines vary by program and are often rolling; but early application is encouraged. See the Fellowship Listings for complete information.
I have financial needs that necessitate a higher salary than just the usual PGY-6 level. Will I be able to earn additional income during the advanced second year fellowship?
Many of the advanced fellowships allow or even require work as an attending anesthesiologist, and many do offer salaries above PGY-6 level. See the Fellowship Listings for details.
I am interested in doing a Research fellowship and I have heard that there is a program from the National Institutes of Health for loan repayment for researchers. Do you have details?
For the Research fellowships, the National Institutes of Health Loan repayment program may be available, which pays up to $35,000 in student loan debt for every year of research. Details are available at http://www.lrp.nih.gov/index.aspx.
Can I apply for a second year advanced fellowship at a different institution than the one I am currently in for my first year ACGME Pediatric Anesthesia fellowship?
Yes, most of the advanced fellowships are open to applicants from outside institutions. See the Fellowship Listings for details.
Will the advanced second year fellowship help me get a good job in Pediatric Anesthesiology?
In the increasingly competitive job market for Pediatric Anesthesiology, the Pediatric Anesthesia Leadership Council feels that the specialized expertise of the second year advanced fellowship is a distinct advantage, and many departments in leading hospitals are giving preference to these candidates.
Will there be additional second year advanced fellowship institutions and fellowships in the future?
We anticipate that several more institutions that are developing advanced fellowships will formally join the network in the next several years. In addition, programs already offering some second year advanced fellowships are likely to add additional programs and fellowship positions.
Will there be additional fellowship areas added in the future?
We are continuing to evaluate the possibility of offering second year advanced fellowships in Critical Care, OR Management/Leadership, and Global Health; but these will not be offered for the first year of the network. These programs may be already offered by some institutions; contact the Program Director listed on the Fellowship Listings for further details.
![]()
The Human Resources for Health Program in Rwanda
Craig D. McClain, MD, MPH, FAAP
Boston Children’s Hospital and Harvard Medical School
Marcel E. Durieux, MD, PhD
University of Virginia School of Medicine
Jennifer E. O’Flaherty, MD, MPH, FAAP
Dartmouth-Hitchcock Medical Center
Rwanda is a small country in east-central Africa that conjures up many disturbing images for Americans. Those things are part of history now and the reality is that when one thinks of Rwanda, ideas such as stability, safety, resilience, financial growth and hope should be foremost. Despite the potential for a bright future, medical care is severely lacking. Specifically, there are almost 11 million people in Rwanda and there are currently only 11 MD anesthesiologists to serve the entire population. Anesthesia technicians, who essentially have the equivalent of a high school education, deliver most anesthetics in Rwanda.

Front entrance to the main teaching hospital, Centre Hospitalier Universitaire de Kigali (CHUK), in the capital city of Kigali.
Most of the MD anesthesiologists are located in the larger cities. This results in nearly all the anesthetics in the rural district hospitals and most in urban areas being administered by unsupervised anesthesia technicians. In addition to the obvious lack of adequate human resources, there are also significant issues with physical resources such as equipment and drugs.
Some of the wonderful children of Rwanda.

An anxious patient.
In an effort to improve the overall state of medical care in Rwanda, the Rwandan government has enacted a bold new approach to capacity building and creation of a self-sustainable medical care system. This plan is called the Human Resources for Health in Rwanda (HRH) program. This is a US government funded program, led by the Rwandan Ministry of Health (MOH) that will provide funding for seven years (until 2019) to place US physicians, nurses, dentists and logisticians in Rwanda to educate Rwandan trainees and provide mentorship for Rwanda practitioners. The physician component of this plan involves anesthesiologists, surgeons, internists, pediatricians, obstetricians, gynecologists, family practitioners and emergency physicians.

A Glostavent anesthesia machine
manufactured by Diamedica
The Rwandan MOH has contracted with several medical schools in the U.S. to recruit faculty to live in Rwanda for two months to one year (depending on subspecialty experience) to train Rwandan residents and offer mentorship to existing Rwandan faculty. The Clinton Health Access Initiative is helping to provide administrative and organizational support. This first group of physicians was deployed to Rwanda in August 2012. The program is planned to last until 2019 when the U.S. faculty will be phased out, as the Rwandan physicians will be able to support the training programs without expatriate human resources.
As mentioned, Rwanda is a very safe place to live and work. There are no travel restrictions or warnings in place from the U.S. Department of State. The anti-corruption watchdog group, Transparency International, rates the Rwandan government as among the least corrupt in all of Africa.
There are currently two anesthesiologists working in Rwanda as part of HRH and we expect to send up to five per year. There is a particular need for expertise in pediatric anesthesiology as a significant number of patients seen in the operating theater are children. Participating faculty will receive salary and benefits commensurate with their time commitment. We want to make all members of SPA are aware of this program and encourage interested anesthesiologists to contact the HRH program via email at anesthesia@rwandahrh.com. You can also visit the website http://rwandahrhprogram.wikispaces.com for more information about participating.
![]()
Lifebox Campaign Raises Awareness (and funds!) for Safe Pediatric Surgery Worldwide
Lifebox fundraising campaign targets pediatric pulse oximeters
Ann Hau, MD
Texas Children’s Hospital
Photos ©Copyright Lifebox Foundation
The gift of giving was in full swing this past holiday season in the Department of Anesthesiology at Texas Children’s Hospital in Houston, Texas. Faculty, trainees, and CRNAs from the department joined together to raise $3,900 in four weeks for the Lifebox Foundation, the non-profit organization that aims to improve safe surgical conditions worldwide. The fundraising campaign, which is the first to focus on pediatric pulse oximeters, will provide 13 pediatric pulse oximeters to resource-poor countries.
SPA president, Dr. Nancy Glass, initiated the Lifebox donation campaign at Texas Children’s Hospital, her home institution, after hearing about similar efforts from other programs. Faculty and residents in anesthesiology departments across the country, including University of Florida, Beth Israel Deaconess Medical Center, and Duke University, have conducted successful fundraising campaigns for Lifebox. However, no other initiative, until now, has focused on raising awareness and funds for pediatric probes. “I’ve seen disposable pulse oximeters, particularly in the postoperative recovery areas, that have been used literally hundreds of times, and are taped on, wrapped around multiple ways. Oftentimes, for pediatric patients, the probes are not the appropriate size,” Glass describes.
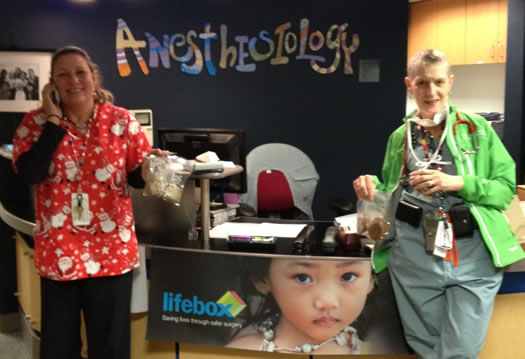
Dr. Nancy Glass (right) and a colleague at a Texas Children’s Department of Anesthesiology bake sale to rase funds for Lifebox.
Glass was particularly interested in Lifebox’s efforts in Central and South America, where several faculty members from Texas Children’s participate in mission trips. Her own work in Antigua, Guatemala over the past decade has exposed the challenges of caring for pediatric patients in a resource-limited environment.

A mother and baby in Ethiopia.
Dr. Sudha Bidani, assistant professor at Texas Children’s Hospital, will utilize one of the newly donated pulse oximeters from Lifebox in her upcoming mission trip to Portoviejo, Ecuador. “There are no pulse oximeters, period,” Bidani says, regarding her experiences at the Central and South American hospitals where she conducts missions. In the past, Bidani has had to collect used pediatric probes for her medical mission trips.

A C-Section underway in Kibagabaga.
In addition to use in the intra- and peri-operative settings, the pulse oximeter from Lifebox has been identified as an important innovation in newborn health in resource-limited settings (Thairu, et al.) To date, Lifebox has distributed 1,200 pediatric probes around the world to hospitals and through organizations like Smile Train and East Meets West. The team has also started sending out additional pediatric probes along with their oximeters to areas that may need them. Forty pediatric probes have been sent to Liberia for an upcoming training program. Tutorials for neonatal patients, which will be available on Lifebox’s website and on the device’s accompanying educational DVD, are also in the works.

A young patient in the Phillipines.
There is no doubt that the mission to improve safe pediatric surgery worldwide will require ongoing collaborations with organizations like Lifebox. Other pediatric anesthesiology groups, both private and academic, can take note of TCH’s efforts and join the challenge to create safer surgical conditions for the global pediatric population.
“I think we can do even more,” Glass says. “I would love to see us do more to make a difference.”
For more information, or to join the Lifebox challenge and match – or even better – TCH’s fundraising efforts, or for more information, please contact info@lifebox.org or call on 0203 286 0402.
References:
Thairu, L., et al. Innovative newborn health technology for resource-limited environments. Tropical Medicine and International Health. 2013;18(1):117-128.
![]()
Juvenile Diabetes: An Update
Kimberly K. Nesbitt MD
Vanderbilt University
Juvenile Diabetes is on the rise, but research efforts are waging a valiant response. With diabetology being such a dynamic field, it is helpful for the anesthesiologist to be aware of progress in diabetes research and management. Type I Diabetes (Juvenile Diabetes), is purely an autoimmune disease, unlike Type 2 which may become insulin requiring. All efforts are directed at conquering the antigen-antibody cycle. Three major research groups are spanning the continents in efforts to improve the study numbers while covering a multi-cohort population. The studies are primarily covered by individual focus groups, allowing concentrated efforts and outcome directed focus, on disease variables and treatment options.
The Juvenile Diabetes Research Foundation (JDRF) has focused its efforts on increasing public donations while lobbying actively in Washington for federal support. Their primary research attention is on the cellular milieu that would allow an artificial pancreas to provide glucose/insulin homeostasis. JDRF is also intimately connected with Trial Net (TN), an international study group involving centers throughout the United States, Canada, and Europe. JDRF is the primary sponsor of four groups, while the NIH funds 14 North American Sites. Trial Net is the umbrella network for prevention directed studies, while also being focused on identifying most effective interventions. Entry into the study is through family risk screening.
Multiple genes that predispose a person to disease progression have been identified. It is a trigger event or multiple trigger events that, in conjunction with genetic predisposition, allows gene expression and determines progression rate to disease. Type 1 diabetes is caused by Beta cell directed antibodies that specifically target the insulin producing cells, normally autoregulated by the pancreas. Predisposition does not guarantee progression to disease, but the number of antibodies present can stratify the risk of developing the disease and the time to disease presentation. Researchers have met with success in identifying a number of pathways to prevention or delay of disease development. Moderate risk patients are those 50% likely to manifest the disease, while high risk patients are 85% likely to do so. On the treatment/prevention side, desensitization with small doses of oral insulin has shown promise. Inhibition of T cell activation is being studied in the Abatacept trials. Future treatments utilizing combination therapy are on the horizon. These include anti-inflammatory, immunomodulatory (B and T cell) and antigen specific agents, as well as, immunologic expansion and mitogenic stimulation.
DPT I is a precursor study. Antibody activity and disease confirmation is the focus of work at the Barbara Davis Center, University of Colorado. George Eisenbarth is the father of this research community. From the work of his team, we know that it can take up to 10 years from the coupling of genetic predisposition and trigger events to actual diagnosis of Type 1 diabetes. The most common age of diagnosis is in the 8-14 age cohort. Of interest, however, is the fastest growing cohort. This is the 1-4 age cohort, indicating a rise in disease incidence with a decrease in time from coupling to disease manifestation. Their data stratified risk according to number of antibodies identified. No disease or risk elevation was identified with 0-1 antibodies. Identification of two or three antibodies increased the risk to a 35% chance of disease diagnosis within 5 years. Four or more antibodies carried a 50% risk of disease presentation within 5 years, but a 100% lifetime risk for disease.
Although genetic predisposition is a key factor, 90% of Type 1 patients have no knowledge of a specific family member w IDDM at the time they are diagnosed.
The Type I Diabetes Exchange, founded in 2011, through generous funding of the Leona M. and Harry B. Helmsley Charitable Trust is an integrated model that includes a clinic-based registry and bioregistry that is used to direct efforts in identifying those treatments and management techniques associated with good A1Cs and lower morbidity. Finding an A1C of 8.5 in a young child is considered acceptable, but it would not be considered optimal control in an adult. Physiological changes in growth and development can cause unpredictable changes in insulin requirements. Juvenile diabetes requires individualized management but can we individualize the care during anesthesia and surgery? Based on outcome markers, the study group is focused on identifying the most successful care practices. Thus they ask the question, “If they are doing well, they are doing what?” Information is gathered through chart review, survey, outcome evaluation, data collection and is shared. This organization even has a social network for Type I diabetics where individuals can share information. More information can be found at www.T1Dexchange.org.
What about our perioperative care of the Type 1 patient? In recent studies, we have learned that tight control of blood sugar may lead to undesirable hypoglycemia. Children are even more vulnerable to hypoglycemia. However, we must also anticipate the elevation of blood sugar associated with perioperative stress and surgical trauma. So what do we do? Most anesthesiologists would agree that hyperglycemia is of concern and many use greater than 200 as the threshold for intervention. Juvenile diabetes requires individualized management but can we individualize the care during anesthesia and surgery? What do we do with a patient on an insulin pump? Do we convert all our patients to a sliding scale? How reliable is a patient’s continuous glucose monitoring(CGM)? Are we still converting all diabetic management in the operating room to a sliding scale regimen? Can we utilize the patients ongoing management protocol to judge insulin response and blood sugar trends? A number of papers have provided suggestions for more individualized management of the pediatric diabetic.
Chadwick and Wilkinson presented their review for Diabetes Mellitus and the Pediatric Anesthetist in Pediatric Anesthesia, 2004. It provided a concise overview of the pathophysiology in Type I Diabetes and offered recommendations for perioperative management, taking into account the metabolic impact of anesthesia and surgery on these patients. It was followed by another article, this one by Rhodes, Ferrari and Wolfsdorf in Anesthesia & Analgesia (2005) entitled Perioperative Management of Pediatric Surgical Patients with Diabetes Mellitus. These authors simplified the management dilemmas and included specific flow diagrams for patients receiving one of several management schedules and individualized them to the main groups of split insulin regimens (long/short insulin therapy), single long acting insulin regimens and patients controlled with the use of an insulin pump. How did we receive this information? Did our practice change accordingly? In 2009, the ISPAD Clinical Practice Consensus Guidelines Compendium was published in Pediatric Diabetes.
Certainly we have the data and recommendations for specific protocols but how are we doing with our blood sugar targets perioperatively? Studies are needed specific to the operating room arena looking at the benefit of utilizing these protocols or the results of not utilizing individualized therapy for surgery. There is plenty of room for other focused outcome studies in the pursuit of best management for our diabetic patients.
Type II Diabetes: A new challenge for pediatric anesthesiologists
Anuradha Patel, MD FRCA
NJ Medical School, Newark NJ
The worldwide prevalence of diabetes is on the rise not only in developed countries, but also in developing countries. Based on the 2011 National Diabetes fact sheet from the Centers for Disease Control, the prevalence of diabetes is 25.8 million children and adults in the United States. In 2010, about 215,000 people younger than 20 years had type I or type II diabetes in the US, which translates to 1 in 400 children and adolescents. The SEARCH for Diabetes in Youth Study (www.searchfordiabetes.org) estimates that about 3,700 youth under 20 years old are diagnosed with type II diabetes each year, and the disease is particularly prevalent in minority youth. Insulin dependent or type I diabetes is more common in pediatric patients under 10 years but the incidence of type II diabetes in the older child is increasing due to the epidemic of obesity in children.
Complications, morbidity, and mortality associated with diabetes are all likely to occur earlier in patients who develop the disease early in life. Further, children of women with type II diabetes are more likely to develop the disease. Thus, the burgeoning of diabetes in younger populations could lead to a vicious cycle of ever-growing rates of diabetes.
Pediatricians and other physicians may feel ill-equipped when faced with the challenge of treating the rapid emergence of an adult disease in children and adolescents. The American Academy of Pediatrics has developed a clinical practice guideline to provide evidence-based recommendations on managing 10- to 18-year-old patients in whom type II DM has been diagnosed. Type II DM is associated with insulin resistance in children and adolescents. To date, metformin is the only oral agent approved by the FDA for use in children. Type II diabetic children are more likely to be on insulin therapy as metformin alone may be inadequate in achieving sustained glycemic control in children. The National Institute of Diabetes and Digestive and Kidney Diseases–supported Treatment Options for type II diabetes in Adolescents and Youth trial (TODAY trial) found that addition of rosiglitazone to metformin provides superior glycemic control, but rosiglitazone is not FDA approved.
In addition, adherence to diet control and oral therapy is a major problem in adolescents. When the decision is made to use insulin, sustained glycemic control in children with type II DM can be obtained in majority of patients with single bedtime long-acting insulin. There may be some risk of hypoglycemia (overnight or fasting) and hyperglycemia with this regimen during the day for which short-acting insulin before meals may be needed in some patients.
The advent of continuous insulin delivery devices, long- and rapid-acting insulin analogs, and other technological advances in diabetes care have made the management of perioperative blood glucose levels a greater challenge for pediatric anesthesiologists. Pediatric anesthesiologists must consider a child’s metabolic control, age, size, pubertal development, the intended surgical procedure, and its length when devising a perioperative plan. In addition, the type II diabetic child will have the challenges of the obese child, such as difficult IV access, possibly intubation difficulty, psychological immaturity, etc. It is important to note that the insulin dose for children varies with age of the child, pre-pubertal children are relatively more sensitive to insulin than pubertal adolescents.
General principles of management for diabetic patients include the following:
- Thorough preoperative assessment by the anesthesia and endocrine services is needed for optimization and establishment of goals for glycemic control.
- Metformin needs to be discontinued 24 hours before a procedure because of its long half-life and the risk of lactic acidosis in the setting of dehydration, hypoxemia, or poor tissue perfusion.
- Diabetic patients should be scheduled as the first case in the morning so that prolonged fasting is avoided and diabetes treatment regimens can be most easily adjusted.
- Blood glucose measurement before anesthesia is mandatory. If the surgery has to be delayed for any reason, frequent blood glucose monitoring will be needed to prevent hypoglycemia or severe hyperglycemia.
- On the morning of surgery, no rapid- or short-acting acting insulin is given unless the blood glucose is >250 mg/dL. The regimen for managing diabetes before, during, and after a surgical or diagnostic procedure that requires the child to fast should aim to maintain near-normoglycemia.
- A reasonable and achievable goal for blood glucose is a range of 140-180mg/dl. This will reduce the risk of osmotic diuresis, dehydration, electrolyte imbalance, metabolic acidosis, infection, and inadvertant hypoglycemia.
- For patients with type II diabetes who are not treated with insulin (but are insulin resistant), an insulin dose of 0.1 U/kg of rapid-acting insulin may be administered subcutaneously to correct blood glucose >250 mg/dL.
- Patients undergoing major surgery and those on insulin pumps should have intravenous insulin and glucose regimens. Regular insulin should be used for IV infusions.
- Management of the child on an insulin pump depends on the duration of the surgical procedure. Those having minor procedures expected to last for <2 h can usually continue to receive insulin via their pump with their usual basal rate for that time of day. For procedures expected to last more than 2 h, transition to an IV insulin infusion is recommended.
Pediatric patients with diabetes are managed with increasingly complex and changing regimens. A thorough and useful review with standardized algorithms are presented in a paper from Children’s Hospital Boston for the management of pediatric patients with either type I or II diabetes mellitus presenting for surgery and general anesthesia.
The goals of glycemic control during the perioperative period and in critically ill patients have been the subject of intense study and much controversy. It is well known that hyperglycemia may have deleterious short-term as well as long-term consequences. Hyperglycemia can adversely affect fluid balance (through glycosuria and dehydration), impair wound healing and increase the risk of surgical site infections by inhibition of neutrophil function.
The results from clinical studies have not been consistent on the relationship between perioperative glycemic control and short-term risk of infection or morbidity. Most studies have been in adult patients undergoing major surgery or in critically ill patients in the intensive care unit. In one of the few pediatric studies after cardiac surgery, it was found that tight glycemic control can be achieved with a low hypoglycemia rate but it does not significantly change the infection rate, mortality, length of stay, or measures of organ failure, as compared with standard care. Meta-analysis of randomized trials in critically ill patients suggests that there is no benefit to tightening glycemic control to normal levels compared to a goal of 140-180mg/dl, to reduce the risk of inadvertant hypoglycemia. It remains to be seen if there is benefit of tight glucose control once hypoglycemia is minimized with technological advances such as continuous glucose monitoring systems.
As diabetes treatment options for children continue to change, the involvement of anesthesia, surgery, and endocrine services to systematically address issues in co-management of pediatric surgical patients with type II DM will lead to best outcomes.
Copeland KC, Silverstein J, Moore KR et al, Management of Newly Diagnosed Type 2 Diabetes Mellitus (T2DM) in Children and Adolescents. Pediatrics 2013;131(2):364-82.
Rhodes ET, Ferrari LR, Wolfsdorf JI, Perioperative Management of Pediatric Surgical Patients with Diabetes Mellitus. Anesth Analg 2005; 101:986-99
![]()
Pheochromocytoma – Understanding Perioperative Management for the Pediatric Patient
ES Williams, MD
Texas Children’s Hospital
What is Pheochromocytoma?
Pheochromocytoma is a condition that involves a tumor of the sympathetic nervous system or tumors in multiple locations that secrete catecholamines. The catecholamines secreted are typically norepinephrine, epinephrine and sometimes dopamine. The adrenal medulla houses cells known as chromaffin cells that secrete the hormones. It is these cells that are the sources of the excess catecholamines. Typically pheochromocytoma is located in the adrenal gland, however, it can be located in extra adrenal areas such as the gland of Zuckerandl (located near the bifurcation of the aorta), the GI tract, the thorax, or bladder.
Of note, in children, the tumors are usually not located in the adrenal glands but in the other areas such as the thorax and are less likely to secrete the catecholamines. There are more multiple, extra adrenal and bilateral pheochromocytomas in pediatric population than compared to adults.
Since the institution of alpha-blockade preoperatively, the operative mortality has greatly decreased from > 50% to now less than 3%.
How common is pheochromocytoma?
This is a rare condition that occurs in approximately 2-8 people per 1 million. It is even more rare in children occurring in 0.2 people per million.
What are the signs and symptoms?
The classic triad of headache, diaphoresis and palpitation occurs in up to 90% of patients with pheochromocytoma. Interestingly, nausea can also be present in children. Other symptoms include fatigue, weight loss, abdominal pain, visual disturbances, pallor and anemia.
Sustained hypertension (HTN) is more common in children while paroxysmal HTN is more common in adults. If the HTN remains untreated the patient can have severe complications such as heart failure, cardiomyopathy, stroke, shock or pulmonary edema.
How is this test diagnosed?
Typically patients are diagnosed using the 24-hour urinary excretion of catecholamines and metabolites or the assay for plasma catecholamines and metabolites. The measurement of urinary catecholamines is considered the most sensitive test in children. There exists other tests such as the clonidine suppression test or glucagon stimulation test that are used when results from urinary or plasma hormone levels are equivocal. Once the results of the assays indicate the presence of catecholamine excess, the location of the tumor is determined using either CT or MRI. When tumor location remains in question I-metaiodobenzylguanidine (MIBG) scintography can be performed.
How do I optimize my patient preoperatively?
Once it is determined that a patient has pheochromocytoma, it is imperative to institute a multidisciplinary approach that focuses on optimization of the patient’s hemodynamics and electrolytes prior to surgery.
Lab work should include a metabolic panel, complete blood count and type and cross for blood products. Be watchful for hypokalemia due to hypereninemia and secondary hyperadlosteronism. Also, hypercalcemia, and hyperglycemia may be present.
An electrocardiogram and echocardiogram are also necessary.
In order to obtain normotension, alpha blockade must be initiated. Typically the non-competitve alpha-1 receptor antagonist phenoxybenzamine (0.25-1 mg/kg/day)is administered. This drug allows the blood pressure to be lowered by blocking the vasoconstrictive effects of the cathecholeamines. The drug may take several days to several weeks to obtain normotension. Phenoxybenzamine is long acting requiring twice daily dosing. Once the patient has blood pressures normalized, no signs of ST-T wave changes on EKG, and no arrhythmias, then institution of a beta-blocker can be started. It is imperative that beta blockade never be initiated prior to the start and successful titration of the alpha blockade as to prevent a hypertensive crisis due to unopposed vasoconstriction.
It is also important to remember that the long duration of action of phenoxybenzamine can predispose the patient to hypotension once the tumor has been excised.
What is the appropriate intraoperative and postoperative management?
Once the patient is deemed optimized for surgery, it is imperative that the anesthesiologist understands the overall tumor physiology and understands the potential hemodynamic changes that occur intraoperatively and postoperatively.
First, prior to entering the operating room the anesthesiologist must work to avoid patient fear and stress; these emotions work to increase the patient’s blood pressure. Additionally it is prudent to avoid drugs that may cause negative hemodynamic changes such as morphine and atracurium, which cause histamine release and possible subsequent release of cathecholeamines from the tumor. Other drugs to avoid include vagolytic agents such as atropine, pancuronium and succinylcholine. Standard monitoring with invasive arterial blood pressure monitoring is needed. Induction using agents that blunt response to laryngoscopy is crucial. Maintenance with any volatile anesthetic and titrated fentanyl are acceptable. The patient that is undergoing a laparoscopic procedure does not require regional anesthesia however, an open procedure may benefit from epidural analgesia. Again, the hemodynamic changes that can occur demand having vasoactive drugs that can quickly lower the blood pressure such as sodium nitroprusside the preferred vasodilator. Additionally, once the tumor is excised, the potential hypotension that occurs demands aggressive fluid resuscitation, availability of pressors such as norepinephrine, phenylephrine, and dopamine. Once the tumor is removed, the patient can experience hypoglycemia, thus, institution of dextrose containing solutions may be required.
Finally, the most important aspect of perioperative management of the pediatric patient with pheochromocytoma is awareness of the hemodynamic changes that occur and vigilance to prevent and or treat such derangements.
Sources
- Hack HA The perioperative management of children with pheochromocytoma Pediatrics Anesthesia 2000 10 (5) 463-476
- Waguespack SG et al A current review of the etiology, diagnosis and treatment of pediatric pheochromocytoma and paraganglioma Journal of Clinical Endocrinology and Metabolism 2010 95 (5) 2023-2037
- Wall, R Endocrine disease Anesthesia and Co-Existing Disease Stoelting 5th Ed 2008 pp. 388-393
![]()
![]()
Regional Anesthesia and Acute Compartment Syndrome
PRO
Martha Pankovich, MD
Seattle Children’s HospitalOver the past two decades, the use of regional anesthesia in children has expanded to such a degree that it is no longer a luxury performed by a few, but a set of techniques widely practiced in pediatric centers. With the improvement of tools used in children and studies involving large numbers of patients, we know that these techniques are very safe to perform in children, and to perform them under general anesthesia.1-2 We also know from years of experience and research that good regional blocks have a multitude of benefits including a reduction in the overall stress response to surgery, a reduction in the use of anesthetic drugs, greater hemodynamic stability, earlier discharge and overall better pain control for patients during and after surgery. Use of regional anesthesia can reduce the exposure of patients to inhalational agents and narcotics, which may lead to a smoother emergence and less nausea and vomiting. Concerns for long term cognitive effects due to exposure to inhalational agents may also be curbed. A benefit specific to epidural analgesia is earlier return of gut function compared with use of opiates, which slow gut function.3
Strong evidence suggests that regional anesthetic techniques have the potential to influence surgical outcomes by reducing the metabolic, humoral and immunologic responses to the stress of trauma and surgery, although larger, more definitive studies are necessary to prove this benefit.4 Given all the known benefits of regional anesthesia, the questions become, why do so many surgeons refuse to allow a regional block for their patients who are at risk for compartment syndrome? And are we doing right by these patients by denying them the benefits regional anesthesia has to offer?
Acute compartment syndrome (ACS) is a rare complication of limb trauma or surgery, but it is an emergency with potentially devastating complications. The degree of tissue damage and risk of limb loss and even death is directly related to the time from the development of ACS to the performance of a fasciotomy to relieve the pressure and restore blood flow. The most relied upon early warning sign of ACS is pain that is out of proportion to the degree of trauma or surgery. However, this is not always reliable and other signs, such as leg swelling, pulselessness or paresthesias, must alert caregivers to the possibility of ACS. The key to early diagnosis is a high level of suspicion, recognizing the signs and symptoms, and measuring the pressure in the limb compartment at risk.
The concern with using a regional anesthetic technique in patients at risk for ACS is that the superior analgesia will mask pain associated with ACS. This fear has not been supported in the literature. In 12 reported cases of ACS in children with epidural analgesia, all patients had signs or symptoms of ACS. With careful review of those cases, many delays in diagnosis were due to providers not recognizing those signs as potentially ACS, attributing increased pain, for example, to a failure of the analgesic modality.5
Why then is there such a concern about masking ACS? There are few but some definitive reports that can directly link epidural analgesia to masking the signs and symptoms of ACS. However, in a review by Johnson and Chalkiadis, the authors could only find two reports in which epidural analgesia truly masked pain associated with ACS in a lower extremity. In both cases, a dense sensory and motor block was present. Dense motor block with epidural analgesia also may have masked a number of cases of gluteal compartment syndrome reported in several obese adult patients.6 However, the majority of reports of ACS in adult patients with epidural analgesia show that the signs and symptoms of ACS were present.9 The major problem arises when those signs and symptoms are not recognized as such. In addition, no cases of ACS have been associated with continuous peripheral nerve blocks in adults or children, and there are only two reported cases of ACS in a lower limb implicating a single shot peripheral nerve block. In one case, pain was present, and in the other, a femoral nerve block was implicated in calf ACS. A femoral nerve block is unlikely to mask calf ACS given the sensory distribution of the femoral nerve below the knee is only medial.7
The key to using regional anesthesia for patients at risk for ACS is first knowing which patients are at risk, second having staff caring for these patients well aware of the risks and importance of good care of pressure points and patient positioning, and thereby vigilant to any signs suggestive of ACS, and third, using regional techniques responsibly to minimize any risk of masking signs of ACS. If one is working in an environment where close monitoring of these patients is not possible, then a catheter technique for postoperative analgesia may not be the best choice. Otherwise, there is no contraindication to providing a patient at risk for developing ACS with an appropriate regional anesthetic technique. With the risks associated with regional anesthesia being extremely low, it is our obligation to provide the best care for our patients, which includes the best intraoperative and postoperative analgesia.
In several recently published reviews5,6,8 of the use of regional anesthesia and the development of ACS, several important recommendations have been suggested for patients at risk:
- Always weigh the benefits against the risks of providing a patient with a regional anesthetic technique.
- Use low concentrations of local anesthetic to avoid dense sensory and motor blockade. 0.2% Ropivicaine is a good choice.
- Use ultrasound for peripheral nerve blocks. Ultrasound guidance has been shown to allow for use of smaller volumes of local anesthetic. Using smaller volumes will generally allow for a shorter duration of the block.
- For patients with epidural or peripheral nerve catheters it is imperative to have continuous postoperative monitoring to identify any changes in pain or sensation that are unexpected and to alert providers immediately of those changes. If dense sensory or motor block is present, it is imperative to reduce the amount and/or concentration of local anesthetic being administered.
- If epidural analgesia is used, it is essential to place the epidural catheter as close to the involved dermatomes as possible to avoid excessive block of areas not involved in the surgery or trauma. ACS can present as pain remote to the surgical site, for example in a lower extremity after a urologic procedure in the lithotomy position.
- Education of staff about ACS and regional anesthesia is critical for good postoperative care.
- An acute pain team must be available.
- Consider having the surgical and the acute pain teams assess patients together.
Johnson and Chalkiadis stress that vigilance is critical to diagnose patients with ACS early, which is true whether or not a regional technique is used.6 Even when children are placed on opiates for pain control, it still requires vigilance and a high degree of suspicion in order to avoid missing the diagnosis of ACS. In a study published by Bae in 2001, 33 children were diagnosed with ACS over a five-year period.9 None had an epidural placed for postoperative analgesia, and many had a delay in diagnosis despite showing signs of ACS.
There is no absolute contraindication to the use of neuraxial or peripheral nerve blocks in patients at risk for ACS. The above guidelines are useful to avoid masking any signs of ACS and to help assure early diagnosis as well. The benefits of regional anesthesia continue to outweigh the risks in most patients. And the choice of technique, single injection or catheter technique is dependent on patient and provider preference as well as the extent of the surgery being performed. All techniques can be used as long as they are used responsibly and providers maintain a high level of suspicion in those patients at risk, and do not allow the presence of a regional technique to influence their level of suspicion.
References
- Giaufre E, Dalens B, Gombert A. Epidemiology and morbidity of regional anesthesia in children: a one year prospective survey of the French-language Society of Pediatric Anesthesiologists. Anesth Analg 1996; 83: 904–912
- Llewellyn, N and Moriarty, A. The National Pediatric Epidural Audit. Pediatric Anesthesia 2007; 17:520-533
- Bosenberg, A. (2011), Benefits of regional anesthesia in children. Pediatric Anesthesia. doi: 10.1111/j.1460-9592.2011.03691.x
- Wolf, A. R. (2011), Effects of regional analgesia on stress responses to pediatric surgery. Pediatric Anesthesia. doi: 10.1111/j.1460-9592.2011.03714.x
- Mossetti V and Ivani G, Controversial issues in pediatric regional anesthesia, Paediatr Anaesth. 2011 Jul 21
- Johnson DJG and Chalkiadis GA, Does epidural analgesia delay the diagnosis of lower limb compartment syndrome in children?, Pediatric Anesthesia 2009; 19:83-91
- Mannion S. and Capdevila X., Acute Compartment Syndrome and the Role of Regional Anesthesia. Int Anesthesiol Clin. 2010; 48 (4): 85-105
- Dalens, B. Some Current Controversies in Paediatric Regional Anaesthesia, Curr Opin in Anaesth 2006, 19:301-308.
- Bae D, Kadiyala R, Waters P. Acute compartment syndrome in children: contemporary diagnosis, treatment, and outcome. J Pediatr Orthop 2001; 21: 680-688
CON
J. Grant McFadyen, MBChB FRCA
Seattle Children’s HospitalAcute compartment syndrome (ACS) is a potentially devastating cause of permanent disability. Early recognition of the syndrome and expeditious treatment is essential to correct the problem before permanent damage occurs. Delayed diagnosis can lead not only to loss of function in the limb and/or the requirement for amputation, but muscle damage can lead to significant hyperkalemia, acidosis, and myoglobulinuria, acute renal failure requiring dialysis, cardiac arrhythmias and occasionally even death. Catastrophic outcomes are inevitable if fasciotomies are delayed for more than 12 hours, whereas a full recovery is achieved if decompression is performed within 6 hours of making a diagnosis.1 In addition to poor clinical outcome, a delayed diagnosis has medicolegal ramifications. In a closed claims review, defense was always successful when a fasciotomy was performed within 8 hours of the first presenting symptom.2
ACS is an uncommon occurrence in children. A search of the National Pediatric Trauma Registry found a 1% incidence of compartment syndrome in forearm fractures, and a 3.3% incidence in lower leg fractures.3 Most residents in orthopedic surgery and anesthesiology are not likely to see a case of ACS during their pediatric training. Teaching hospitals rely largely on residents to make the diagnosis of ACS, especially out of hours. Patients at risk of ACS are often poorly assessed. In a retrospective study of preoperative medical records of 30 consecutive patients who underwent fasciotomies for ACS in a major teaching hospital, documentation was inadequate for 21 patients (70%).4
Much concern has been expressed in the literature about the possible masking of some of the clinical signs of ACS by regional anesthesia,5-7 and even by PCA opioids.8 No randomized controlled trials of patients at risk of ACS have been performed comparing outcomes between those who received a regional anesthetic technique and those who did not. Clinical practice is guided by case reports and retrospective case series.9 Interestingly, to date all the case reports apart from one have been published in surgical and trauma journals.10 Mannion and Capdevila ask, “Does this imply that anesthesiologists are unwilling to publish complications of their techniques or perhaps is there a misunderstanding by surgeons of the exact analgesic and anesthetic effects of modern neural blockade?”.11 The latter may well be true. In an early case report, one of the authors of which is an influential figure in worldwide orthopedic trauma education, a “3-in-1” femoral block was blamed for causing the diagnosis of ACS in the lower leg to be missed.7 However, all four of the muscle compartments of the lower leg are supplied by the sciatic nerve, which was not blocked. The error in blaming the block was pointed out by another orthopedic surgeon (married to an anesthesiologist!).12 The tragedy in this case, however, is that the diagnosis of ACS was delayed because neurological symptoms or pain were erroneously attributed to the regional technique.
The clinical findings of ACS are classically described as the “6 P’s” (Table 1). The earliest and most reliable clinical symptom and sign of ACS is thought to be increasing pain and pain on passive stretching of the muscles within the affected compartment.13 Data from a review of prospective clinical trials assessing diagnosis and outcome of ACS in lower leg injury confirms the limitations of relying on a single symptom to diagnose ACS.14 It was found that overall the sensitivity of clinical assessment was <20% (range: 13% to 19%) for a single clinical finding. The documentation of three or more clinical findings (“P’s”) is required to increase the probability of detecting ACS to 93%. Paresthesias or paralysis may be attributed to a regional technique, and pain may be attributed to failure of a regional technique. Even if the assumption that the symptoms are associated with the regional technique is erroneous, delays in diagnosing ACS commonly occur as a result. Diagnosis of compartment syndrome in the pediatric population is particularly difficult. Apprehension, poor cooperation and difficulties with communication complicate the clinical evaluation of children.
In a case report in Pain Medicine of ACS in the lower leg after elective proximal tibia osteotomy, the authors conclude that “despite concerns of masking pain that may be secondary to compartment syndrome, this case demonstrates that compartment syndrome can be diagnosed in the presence of effective regional anesthesia”.10 This belief is held by many regional anesthesia experts. In this case, however, delayed diagnosis of ACS resulted: severe (10/10 VAS pain score) pain on the second postoperative day, after discontinuation of the femoral and sciatic peripheral nerve catheters, was treated with ropivacaine boluses through the catheters and recommencement of the ropivacaine infusions. There was a seven hour delay before the diagnosis of ACS was suspected by the acute pain service and the orthopedic service was informed.
Objective means of detecting ACS, such as near infrared spectroscopy, T1-weighted MRI and Doppler flowmetry, have not been shown accurately to detect early onset ACS.1,15 The most commonly used objective method in clinical practice is the measurement of intracompartmental pressures. Unfortunately, difficulties remain in the interpretation of findings and their clinical relevance.16 One difficulty is determining the critical pressure level at which muscle compromise occurs. Earlier suggestions of an absolute pressure as the threshold at which to perform fasciotomy made no allowance for the role of blood pressure in maintaining tissue perfusion. Increasing evidence supports the concept of the threshold being a differential pressure. This differential is known as the δ pressure and is the diastolic blood pressure minus the intracompartmental pressure.16 Children have a lower blood pressure, and a higher normal intracompartmental pressure than adults, increasing their risk of ACS.17 It has been suggested that vasodilation caused by regional anesthesia can increase intracompartmental pressure.18 Hand-held needle manometers are not suitable for use in children because they require painful percutaneous needle punctures. Catheters placed at the time of operation can be used to measure intracompartmental pressures using standard manometry, but these can become blocked by fragments of tissue or clots.
The use of regional anesthesia in patients at risk of compartment syndrome continues to be a controversial issue. Denying children adequate pain relief after painful surgery in the name of diagnosing a rare complication seems cruel. It is prudent to suggest that, rather than adopting an “all or nothing” approach to regional anesthesia, surgeons and anesthesiologists should agree on a regional technique which provides analgesia without rendering a limb insensate with a complete motor block. Ropivacaine 0.2% is a wise choice of local anesthetic, both for single shot nerve blocks and post-operative peripheral nerve catheters. Patients at risk of ACS should be regularly examined by the orthopedic service and the acute pain team. A high level of vigilance for symptoms and signs of developing ACS should be maintained. This will avoid erroneously attributing neurological symptoms to a regional technique or increasing pain to a block “wearing off” or “not working”. A good hospital system should be able to provide good postoperative analgesia while at the same time avoiding delays in diagnosis of ACS, with potentially devastating consequences for the patient and the hospital.
References
- Elliott KG, Johnstone AJ. Diagnosing acute compartment syndrome. J Bone Joint Surg 2003; 85 (5-B):625-632.
- Bhattacharyya T, Vrahas MS. The medical–legal aspects of compartment syndrome. J Bone Joint Surg Am 2004;86-A:864–8
- Grottkau BE, Eppsb HR, Di Scala C. Compartment syndrome in children and adolescents. J Pediatric Surgery 2005;40:678-682
- Cascio BM, Wilckens JH, et al.. Documentation of acute compartment syndrome at an academic health-care center. J Bone Joint Surg Am 2005;87:346-50
- Davis ET, A. Harris et al. The use of regional anaesthesia in patients at risk of acute compartment syndrome Injury, Int. J. Care Injured 2006;37:128-133.
- Thonse R, Ashford RU et al. Differences in attitudes to analgesia in post-operative limb surgery put patients at risk of compartment syndrome. Injury, Int. J. Care Injured. 2004;35:290-295.
- Hyder N, Kessler S et al. Compartment syndrome in tibial shaft fracture missed because of a local nerve block. J Bone Joint Surg [Br] 1996;78-B:499-500.
- Harrington P, Bunola J et al. Acute compartment syndrome masked by intravenous morphine from a patient-controlled analgesia pump. Injury, Int. J. Care Injured 31;2000:387-389.
- Mar GJ, Barrington MJ, McGuirk BR. Acute compartment syndrome of the lower limb and the effect of postoperative analgesia on diagnosis. Br J Anaesth. 2009;102:3–11.
- Cometa MA, Esch AT, Boezaart AP. Did continuous femoral and sciatic nerve block obscure the diagnosis or delay the treatment of acute lower leg compartment syndrome? A case report. Pain Medicine. 2011;12:823-828.
- Mannion S, Capdevila X. Acute Compartment Syndrome and the Role of Regional
Anesthesia. Int Anes Clinics. 2010;48(4):85-105.- Eyres KS, Hill G, Magides A. Compartment syndrome in tibial shaft fracture missed because of a local nerve block.J Bone Joint Surg [Br] 1996;78-B:996-7.
- Elliott KG, Johnstone AJ. Diagnosing acute compartment syndrome. J Bone Joint Surg 2003;85(5-B):625-32.
- Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are the clinical findings predictive of the disorder? J Orthop Trauma 2002;16(8):572-7.
- Shadgan B, Menon M, O’Brien PJ, et al. Diagnostic techniques in acute compartment syndrome of the leg. J Orthop Trauma. 2008;22:581-587.
- Al-Dadah OQ, Darrah C, Cooper A, et al. Continuous compartment pressure monitoring versus clinical monitoring in tibial diaphyseal fractures. J Trauma. 2006;60:1330-1335.
- Mossetti V, Ivani G. Controversial issues in pediatric regional anesthesia. Ped Anesth 2012;22:109-114
- Olson SA, Rhorer AS. Orthopaedic Trauma for the General Orthopaedist. Clin Ortho Rel Research 2005;433:30–37
![]()
Dr. Kudchadkar Featured on Student Doctor Network Site
One of our members, Dr. Sapna Kudchadkar, was recently featured on the Student Doctor Network (this is a website for premeds, residents, and fellows which provides support and information for career planning). It is a great PR piece for pediatric anesthesiology. Check it out here.
Meet Sapna and other "young turks" at the Saturday evening special reception at the upcoming SPA spring meeting in Las Vegas.
![]()
Exploratory Meeting for Special Interest Group in Anesthesia for Fetal Interventions at SPA/AAP Pediatric Anesthesiology 2013
Debnath Chatterjee, MD
Children’s Hospital Colorado
Fetal surgery is a rapidly growing and evolving discipline. Multiple minimally invasive fetoscopic interventions, EXIT procedures and open fetal surgeries are being performed at major academic centers throughout the world. The anesthetic management of these complex cases has also evolved over the years.
There will be an exploratory meeting for setting up a special interest group in anesthesia for fetal interventions at the SPA/AAP Pediatric Anesthesiology 2013 meeting in Las Vegas, NV. This meeting will include discussions on setting up a database, sharing anesthetic protocols and collaborating on research.
Date: Saturday, March 16, 2013
Time: 4:00 – 5:00 p.m.
Location: Willows Room, Red Rock Resort
Please let me know if you are interested in being at this meeting and joining the special interest group.
Debnath Chatterjee, MD
Assistant Professor of Anesthesiology
Children’s Hospital Colorado/University of Colorado School of Medicine.
debnath.chatterjee@childrenscolorado.org
![]()
Review of Pediatric Anesthesia Articles From the British Journal of Anesthesia 2012
Elizabeth S. Yun, MD
University of Wisconsin School of Medicine
In 2012, the British Journal of Anaesthesia published thirteen articles on a wide range of topics in pediatric anesthesia. This review briefly summarizes these articles and the references are listed at the end.
Four articles highlighted various issues in acute and chronic pain. B.R. Hallett and G.A. Chalkiadis described a case of opiod induced hyperalgesia, defined as increased administration of opiods leading to increase pain perception and sensitivity, hyperalgesia and allodynia in a neonate. The patient was born at 35 weeks and underwent multiple surgeries to correct gastroschisis. During the hospitalization, the patient experienced increased pain and sensitivity to light touch, agitation and tachycardia despite escalating doses of fentanyl and morphine. The pain service was consulted and modified the patient’s pain regimen by stopping the morphine and fentanyl and adding hydromorphone, ketamine, dexamedetomidine and midazolam infusions. The patient experienced significantly decreased pain and sensitivity and was able to be discharged. While there was no clear explanation, the authors speculated that activation of NMDA receptors was the most important cellular mechanism behind opiod induced hyperalgesia.
In a prospective randomized controlled study, JY Mauch et al investigated the hemodynamic changes with test does used in regional anesthesia. 105 patients were randomized to three different test does solutions given intravenously: bupivacaine, bupivacaine and epinephrine, epinephrine only. A positive test dose was defined as >25% T wave change, changes in heart rate by 10 beats and > 15 mmHg increase in systolic blood pressure. The results showed that these changes occurred in the 2 groups with epinephrine containing solutions. T wave and heart rate changes were noted to be age dependent and systolic BP was age independent. The authors concluded that IV epinephrine solutions altered ECG and hemodynamics and multiple variables are needed to accurately detect intravascular injection of local anesthetics. Mohammed et al described the pharmacokinectics of a new form of intravenous paracetamol in children under 16 years of age. Blood samples from 33 patients under 16 were drawn at various time intervals after intravenous administration of a weight dependent dose and analyzed for paracetamol concentration.
This study showed that paracetamol pharmacokinetics followed a two compartment model and total body weight significantly affected the clearance of this drug in children. A.D. Kristensen et al studied the incidence of chronic pain after open inguinal hernia repair. They sent out a questionnaire to 156 patients who had hernia surgery at ages 6 months to12 years and were now 6 to 48 months out from that procedure. They received 98 responses, and only 5 of the responding patients still reported pain. These patients were invited to have a quantitative sensory test to further evaluate their pain. Three patients came for the test and were found to have pinprick hyperalgesia and decreased pressure pain threshold at site of incision. The authors concluded that the incidence of chronic pain after hernia surgery was lower in children compared to adults. However, they felt a prospective study with long term follow up was needed to further investigate this issue.
Several articles examined issues with cardiac anesthesia with possible implications for the management of other complex surgical patients. J Renner et al noted that dynamic variables like pulse pressure variation and stroke volume variation were better indicators of an adult’s response to fluid bolus compared to static variables like central venous pressure and global end diastolic volume. To see if this concept also applied in children, they measured these values in 26 infants undergoing intracardiac shunt repairs at the times during the surgery when the chest was closed. Their findings indicated that pulse pressure variation was the most simple and reliable indicator of an infant’s response to a fluid bolus.
A study by M. Bojan et al retrospectively reviewed their pediatric cardiac cases from 2007-2010 to see if aprotinin or blood products increased the risk of acute kidney injury in the postoperative period. They defined acute kidney injury as a greater than 1.5 fold increase in creatinine levels. They found that patients receiving prophylactic aprotinin did not have a significant association with acute kidney injury (AKI) or AKI leading to dialysis. However patients receiving additional blood products (PRBC, FFP or platelets) had a1.6-3 fold increased risk of AKI and AKI with dialysis suggesting that transfusions carry a significant risk to the patient. The authors did acknowledge limitations with this study including the retrospective nature, changes in practice that were not controlled and a control that was not balanced with the study group.
Another group of papers described the use of new equipment to improve monitoring and care of pediatric patients. O.Raux et al. looked at the using intraoperative transesophageal doppler (TED) to precisely assess an infant’s response to volume expansion. They felt that using this monitor would prevent adverse outcomes in these patients. They studied fifty patients without cardiac dysfunction who had surgery under volatile anesthesia and intubation. The anesthesiologist blinded to the TED gave volume based on the clinical situation and standard monitoring procedure. The TED then collected data before and after the volume expansion. Of all the data collected, the TED derived index stroke volume was shown to predict and follow the response to volume expansion in neonates the best.
L. Triffterer et al described using the ultrasound to facilitate the placement of an intravenous catheter in the great saphenous vein (GSV) in patients less than 12 months. The GSV was selected because its size and depth made it ideal for visualization of the vein. They had high success rate in this patient population although there was a slight decrease in success for patients under the age of six months due to the smaller size of the vein. N. J. Cuper investigated the use of the near-infrared vascular imaging systems (NIRVISs) for arterial line placement. They used this system over 10 months in patients under three years. With this system, a light source transilluminates the puncture site and the signal is processed to show the vessel on the camera. Once the needle pierces the blood vessel, it is obscured due to the blood.
While there was a tendency for fewer attempts at line placement with the system, it was not clinically significant. Based on their findings the authors felt that this instrument did now show clinically significant improvement in arterial line placement.
R. P. Garnier et al looked to see how the Nexfin noninvasive finger cuff correlated with an invasive arterial line in sedated and awake PICU patients. They found that the finger cuff was well tolerated in patients. There was a high level of agreement between both modalities with diastolic blood pressure and mean arterial pressure. However the Nexfin underestimated the systolic blood pressure. The Nexfin appears to be a feasible option in patients although it may not be the best monitor in patients with low systolic blood pressure due to shock or hemorrhage.
The final group of papers covered a variety of topics. E. Bourgeois et al wanted to determine the MAC of sevoflurane that inhibits reflex pupillary dilatation (a subcortical reflex that correlates with pain perception) in 50% of patients or MAC pup. This study prospectively looked at 49 patients (pre and post pubertal) receiving sevoflurane anesthesia and found that the MAC of suppressing RPD was closer in value MAC BAR (the amount of volatile anesthesia needed to suppress autonomic response to nociceptive stimuli in 50% of patients). They noted that pre pubertal patients had an increased MAC pup perhaps due to changes in the cortex and subcortex that occur during puberty.
A. Schmitz et al performed a prospective randomized crossover trial to determine if the amount of clear sugared fluid had an effect of gastric emptying and residual volume. Fourteen patients were randomized to receive either 3 ml/kg or 7 ml/kg of a sugared clear liquid and the gastric volume was measured with an MRI scan before and one hour after ingestion. They found that the subjects receiving the larger volume had a larger residual volume at 1 hour and the smaller volume returned to baseline in the same time. The final article by V Hermans at al examined the effect of dexamethasone doses on PONV and pain in tonsillectomy.
In a prospective randomized double blinded trial, 147 patients were randomized to one of three groups: dexamethasone 0.15 mg/kg at induction, dexamethasone at 0.5 mg/kg, placebo. Both dexamethasone groups decreased PONV. They did not significantly decrease the need for rescue analgesia in the PACU but pain on POD 2 was better controlled compared to placebo. These effects were not dose dependent. The authors concluded that dexamethasone did control PONV and decreased pain on POD 2 and that there was no difference in the effects between the 0.5 mg/kg and the 0.15 mg/kg group.
References
- B. R. Hallett and G. A. Chalkiadis. Suspected opioid induced hyperalgesia. British Journal of Anaesthesia 108 (1): 116–18 (2012)
- J. Y. Mauch, N. Spielmann, S. Hartnack and M. Weiss. Electrocardiographic and haemodynamic alterations caused by three different test solutions of local anaesthetics to detect accidental intravascular injection in children. British Journal of Anaesthesia 108 (2): 283–9 (2012)
- S. Mohammed, T. Engelhardt, G. A. Cameron, L. Cameron, G. M. Hawksworth, A. F. Hawwa,J. McElnay, P. J. Helms and J. S. McLay. Population pharmacokinetics of single-dose intravenous paracetamol in children. British Journal of Anaesthesia 108 (5): 823–9 (2012).
- Kristensen1, P. Ahlburg, M. C. Lauridsen, T. S. Jensen and L.Nikolajsen. Chronic pain after inguinal hernia repair in children. British Journal of Anaesthesia 109 (4): 603–8 (2012)
- J. Renner, O. Broch, P. Duetschke, J. Scheewe, J. Hocker, M. Moseby, O. Jung and B. Bein. Prediction of fluid responsiveness in infants and neonates undergoing congenital heart surgery. British Journal of Anaesthesia 108 (1): 108–15 (2012)
- M. Bojan, S. Vicca, C. Boulat, S. Gioanni and P. Pouard. Aprotinin, transfusions and kidney injury in neonates and infants undergoing cardiac surgery. British Journal of Anaesthesia 108 (5): 830–7 (2012).
- O. Raux, A. Spencer, R. Fesseau, G. Mercier, A. Rochette, S. Bringuier, K. Lakhal, X. Capdevila and C. Dadure. Intraoperative use of transoesophageal Doppler to predict response to volume expansion in infants and neonates. British Journal of Anaesthesia 108 (1): 100–7 (2012)
- L. Triffterer, P. Marhofer, H. Willschke, A. M. Machata, G. Reichel, T. Benkoe and S. C. Kettner. Ultrasound-guided cannulation of the great saphenous vein at the ankle in infants. British Journal of Anaesthesia 108 (2): 290–4 (2012).
- N. J. Cuper, J. C. de Graaff, B. J. Hartman, R. M. Verdaasdonk and C. J. Kalkman. Difficult arterial cannulation in children: is a near-infrared vascular imaging system the answer? British Journal of Anaesthesia 109 (3): 420–6 (2012).
- R. P. Garnier, A. G. E. van der Spoel, R. Sibarani-Ponsen, D. G. Markhorst and C. Boer. Level of agreement between Nexfin non-invasive arterial pressure with invasive arterial pressure measurements in children. British Journal of Anaesthesia 109 (4): 609–15 (2012).
- E. Bourgeois, N. Sabourdin, N. Louvet, F. X. Donette, M. L. Guye and I. Constant. Minimal alveolar concentration of sevoflurane inhibiting the reflex pupillary dilatation after noxious stimulation in children and young adults. British Journal of Anaesthesia 108 (4): 648–54 (2012).
- Schmitz, C. J. Kellenberger, N. Lochbuehler, M. Fruehauf R. Klaghofer, H. Fruehauf and M.Weiss. Effect of different quantities of a sugared clear fluid on gastric emptying and residual volume in children: a crossover study using magnetic resonance imaging. British Journal of Anaesthesia 108 (4): 644–7 (2012).
- V. Hermans, F. De Pooter, F. De Groote, S. De Hert and P. Van der Linden. Effect of dexamethasone on nausea, vomiting, and pain in paediatric tonsillectomy. British Journal of Anaesthesia 109 (3): 427–31 (2012)
![]()
Peds Passport
 By Helen V. Lauro, MD, MPH, FAAP
By Helen V. Lauro, MD, MPH, FAAP
NOTE: Purchase of travel insurance with air evacuation coverage is highly recommended to meeting attendees and their families.
2013
March 14: Las Vegas, Nevada, USA
Congenital Cardiac Anesthesia Society (CCAS) 2013 Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: CCAS, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.ccasociety.org
Email: ccas@societyhq.comMarch 14-17: Las Vegas, Nevada, USA
Society for Pediatric Anesthesia (SPA)/American Academy of Pediatrics (AAP) Pediatric Anesthesiology 2013
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.comMay 2-3: Ghent, Belgium
The First European Pediatric Resuscitation & Emergency Medicine Congress
Tel: +31 (0) 887555555; Fax: +31 (0) 887554702
Information: Secretariat ESPA, c/o Department of Anesthesia, Intensive Care and Emergency Medicine, Wilhelmina Children Hospital/University Medical centre Utrecht Lundlaan 6, Mail stop: KG 02.307.1, PoBox 85090, 3508 AB Utrecht, The Netherlands
Website: http://www.euroespa.org, http://www.prem2013.be
Email: secretary@euroespa.orgMay 17-19: Dallas, Texas, USA
Intensive Review of Pediatric Anesthesia
Tel: (804) 282-9780, Fax (804)-282-0900
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.com
May 20-21: Houston, Texas, USA
Society for Pediatric Sedation Conference 2013: New Frontiers: The Future of Pediatric Sedation
Tel: (804) 565-6354, Fax: (804) 282-0090
Information: Society for Pediatric Sedation, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsedation.org
Email: sps@societyhq.comMay 31-June 2: Aurora, Colorado, USA
VII International Symposium on the Pediatric Airway (ISPA)
Tel: (720) 777-4530; Fax: (720) 777-7266
Information: Ms. Valerie Cassidy, Children’s Hospital Colorado, 13123 E. 16th Avenue, B090, Aurora, Colorado 80045
Website: http://www.pedsairwaysymposium.org
Email: Valerie.Cassidy@childrenscolorado.orgJune 12-15: Rotterdam, The Netherlands
24th Annual Meeting of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC)
Tel: +41 22 9080488, Fax: +41 22 9069140
Information: Kenes Group, Rue de Chantepoulet 1-3, P.O.Box 1726, CH-1211 Geneva 1 Switzerland
Website: http://www.kenes.com
E-mail: info@kenes.comJune 17-20: Stockholm, Sweden
Ninth International Symposium on Pediatric Pain 2013
Tel: +46 8 5465 1500
Information: Congress Secretariat, MCI Stockholm Office, P. O. Box 6911, SE-102 39 Stockholm
Website: http://childpain.org
Email: confirmation-sweden@mci-group.comJune 19-21: Cambridge, United Kingdom
40th Annual Scientific Meeting of the Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI), in conjunction with European Society for Paediatric Anesthesiology (ESPA)
(History of Paediatric Anaesthesia Meeting Symposium precedes main meeting)
Tel: +44 (0) 20 7631 8862, Fax: +44 (0) 20 76314352
Information: APA Administration Office, AAGBI, 21 Portland Place, London, W1B 1YP, United Kingdom
Website: http://www.apagbi.org.uk, http://www.apagbi2013.com.uk
Email: apagviadministration@aagbi.orgJuly 11-14: Myrtle Beach, South Carolina, USA
Pediatric Anesthesia Update
Tel: (800) 222-6927
Information: Northwest American Seminars, P.O. Box 2797, Pasco, WA 99302
Website: http://www.nwas.com
Email: info@nwas.comAugust 22-25: Niagara Falls, Ontario, Canada
Anesthesia Update: Emphasis on Pediatrics
Tel: (800) 222-6927
Information: Northwest American Seminars, P.O. Box 2797, Pasco, WA 99302
Website: http://www.nwas.com
Email: info@nwas.comAugust 23-25: Rosemont, Illinois, USA
Intensive Review of Pediatric Anesthesia
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.comSeptember 5-7: Geneva, Switzerland
Annual Congress of the European Society for Paediatric Anaesthesiology: Geneva 2013
Tel: +31 (0) 887555555; Fax: +31 (0) 887554702
Information: Secretariat ESPA, c/o Department of Anesthesia, Intensive Care and Emergency Medicine, Wilhelmina Children Hospital/University Medical centre Utrecht Lundlaan 6, Mail stop: KG 02.307.1, PoBox 85090, 3508 AB Utrecht, The Netherlands
Website: http://www.euroespa.org
Email: secretary@euroespa.orgSeptember 18-21: Lucerne, Switzerland
3rd European Conference on Pediatric and Neonatal Cardiac Intensive Care
Tel: + 41 (0)22 839 8484
Information: Symporg SA, Rue Rousseau 30, 1201 Geneva, Switzerland
Website: http://www.symporg.com
Email: elaget@symporg.comOctober 11: San Francisco, California, USA
Society for Pediatric Anesthesia (SPA) 27th Annual Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.comOctober 17-20: Manly, New South Wales (NSW), Australia
Society for Paediatric Anaesthesia in New Zealand and Australia (SPANZA) Conference 2013
Tel: +61 2 4973 6573; Fax: +61 2 4973 6609
Information: SPANZA Secretariat, P.O. Box 180, Morriset, New South Wales, Australia 2264
Email: spanza@willorganise.com.au
Website: http://www.spanza.org.au/index.php/news-events/eventsNovember 8-10: Toronto, Ontario, Canada
26th Pediatric Anesthesia Conference
Tel: (416) 813-7654 ext. 28120 (Ms. Michelle Wan) or (416) 813-7445 (Ms. Shue Lin Loo)
Information: Dept. of Anesthesia and Pain Medicine, The Hospital for Sick Children, 555 University Avenue, Toronto, Canada MSG 1X8
Email: li.conferences@sickids.ca, pediatric.anesthesia@sickkids.ca
Website” http://www.cvent.com/events/pediatric-anesthesia-conference/event-summary-916d4a5d9bc942a09178bd7ad27c102a.aspx
2014
March 6: Fort Lauderdale, Florida, USA
Congenital Cardiac Anesthesia Society (CCAS) 2014 Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: CCAS, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.ccasociety.org
Email: ccas@societyhq.comMarch 6-9: Fort Lauderdale, Florida, USA
Society for Pediatric Anesthesia (SPA)/American Academy of Pediatrics (AAP) Pediatric Anesthesiology 2014
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society of Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.comMay 15-16: Leeds, United Kingdom
Association of Paediatric Anaesthetists of Great Britain and Ireland Meeting
Tel: +44 (0) 20 7631 8887, Fax: +44 (0) 20 76314352
Information: APA Administration Office, AAGBI, 21 Portland Place, London, W1B 1YP, United Kingdom
Website: http://www.apagbi.org.uk
Email: apagviadministration@aagbi.org
Footnote:
Please forward all information concerning congresses relevant to
Pediatric Anesthesia to:
Helen V. Lauro, MD, MPH, MSEd, FAAP, SUNY Downstate Medical Center University Hospital of Brooklyn at Long Island College Hospital, Department of Anesthesiology, 339 Hicks Street, Brooklyn, New York 11201.
![]()