
NM-291
A single center experience with Recombinant Factor VIIa and FEIBA following neonatal cardiac bypass surgery.
King A, Winch P, Tumin D, Miller R, Hersey D, Taylor K, Naguib A
Nationwide Childrens Hospital, Columbus, Ohio, USA
Introduction: Bleeding after cardiopulmonary bypass (CPB) in pediatric cardiac surgery is associated with increased morbidity and mortality.1 Patients less than 6 months of age are particularly vulnerable. Their coagulation systems are immature, and a dilutional coagulopathy occurs secondary to their small blood volume compared to the CPB pump prime.2 To restore hemostatic balance, transfusions of blood products and coagulation factors are often required. This is poorly tolerated in children with limited cardiac reserve and such products are associated with significant infectious and noninfectious risks.3
Recombinant factor VII (rFVIIa) and prothrombin complex concentrates, such as Factor Eight Inhibitor Bypassing Activity (FEIBA) can be used to limit bleeding and allogenic blood product exposure after CPB. FEIBA has a similar safety profile for thrombosis as rFVIIa and is less expensive.4 In adults, it is associated with correction of coagulopathy, decreased blood product utilization, and decreased chest tube output.5 In this study, we retrospectively reviewed the safety and efficacy of FEIBA and rFVIIa in children undergoing the arterial switch procedure.
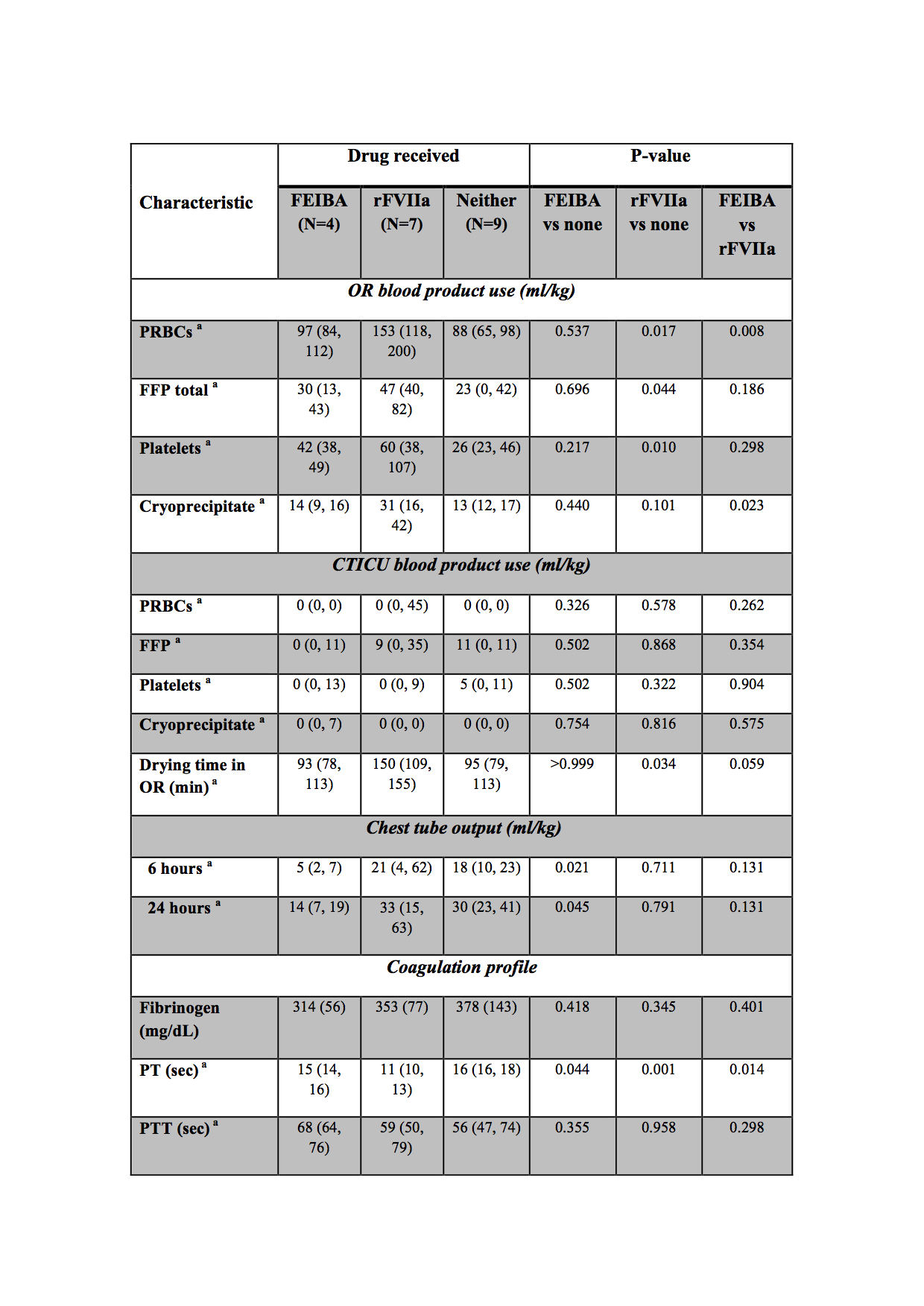
Methods: We reviewed records of children undergoing arterial switch procedures in 2016-2017 at our institution. Patients were classified according to whether they received rFVIIa, FEIBA, or neither drug. Patient and procedure characteristics are described in Table 1. Analyzed outcomes included intraoperative and postoperative blood product use and postoperative chest tube output at 6 and 24 hours. Data analysis included pairwise comparisons among the 3 groups using unpaired t-tests or rank-sum tests for continuous data, and Fisher’s exact tests for categorical data.
Results: Of 17 boys and 3 girls, ages 3-18 days, 4 received FEIBA, 7 received rFVIIa, and 9 received neither drug. Patient and operative characteristics were similar across groups. Intraoperative packed red blood cell and cryoprecipitate administration was reduced in children receiving FEIBA as opposed to those receiving rFVIIa. Postoperative chest tube output was lower in children receiving FEIBA versus neither drug, while using less blood products than those received rFVIIa. There were no differences in the complication profile between the three groups when considering re-exploration (rFVIIa: 1, neither drug: 1) or open sternum (FEIBA: 1, rFVIIa: 4; neither drug: 3). One patient who received neither drug subsequently died .
Discussion: Our data demonstrate a comparable safety and efficacy profile for FEIBA in comparison to rFVIIa, with no major complications in either group. The small number of patients in our cohort and the retrospective nature of the study must be considered prior to reaching any conclusion.
References
1. Paediatr Anaesth. 2005;15:235–40.
2. Pediatr Crit Care Med. 2005;6:348–51
3. Anesth Analg 2012; 115: 364–378.
4. J Cardiothorac Vasc Anesth 2014; 28: 1221-1226.
5. Review of Clinical Outcomes. J Cardiac Surg.2008;23:614-621
-
 NM-291 Image 1
NM-291 Image 1
Top










