
NM-206
Delivery of Anesthesia for Children with Trisomy 18 (Edwards Syndrome): A Review of 49 Anesthetics
1Birmingham M.D. E, 2Diaz m.d, fasa faap C
1Medical College of Wisconsin, Milwaukee, WI, USA; 2Medical College of Wisconsin, Children's Hospital of Wisconsin, Milwaukee, WI, USA
Introduction: Trisomy 18 is the second most common autosomal aberration (1) and encompasses malformations of the nervous, cardiac, respiratory, gastrointestinal, and genitourinary systems. While controversial, with improving survival, larger numbers of infants are receiving operative care. The anesthesiologist must manage the full scope of disease seen in these patients as the cardiac and facial anomalies can make anesthesia especially difficult. Our goal was to describe perioperative complications in Trisomy 18 patients with the largest case series published to date.
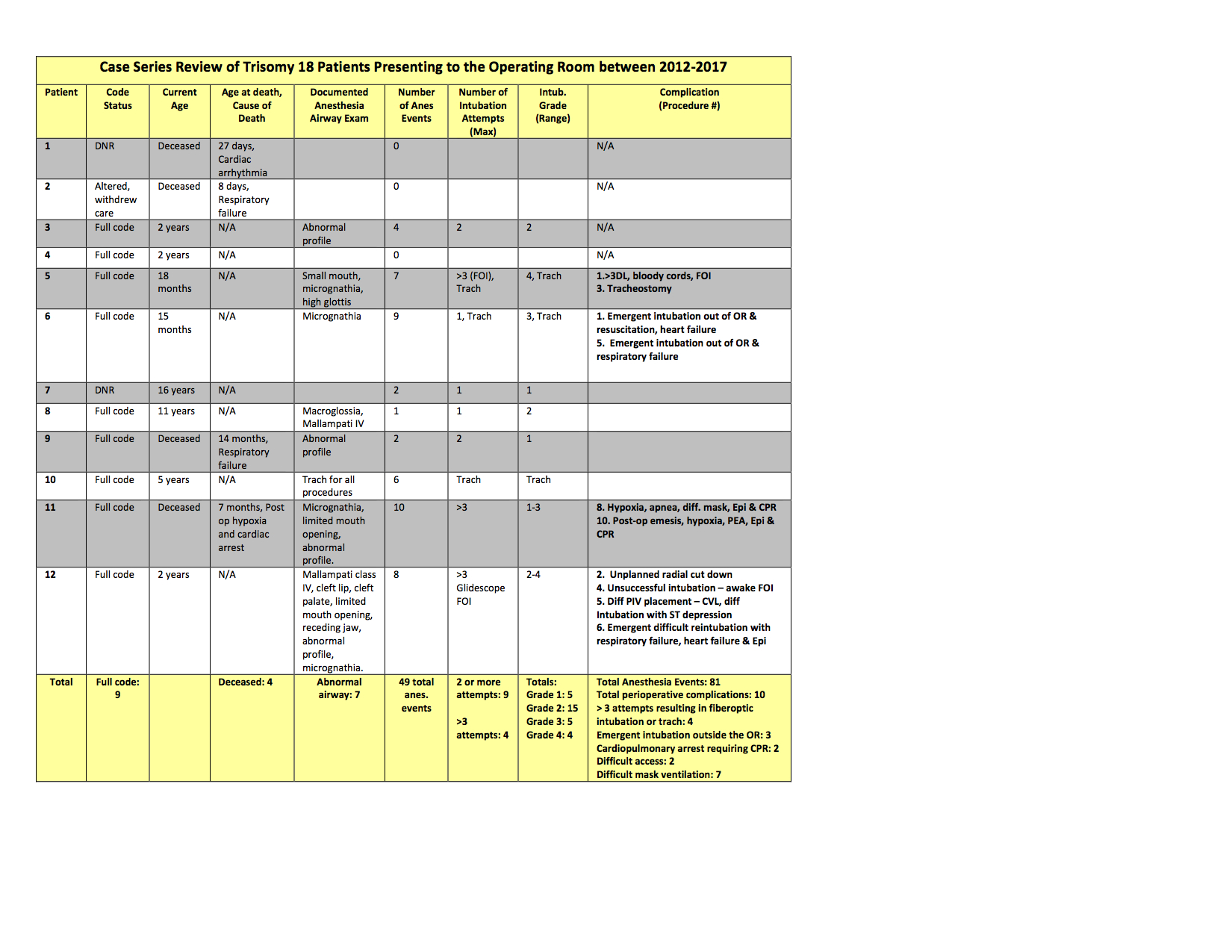
Methods: We performed a retrospective chart review of the twelve Trisomy 18 patients treated at Children’s Hospital of Wisconsin between 2012 and 2017. Anesthesia records were analyzed and comorbidities, ASA status, code status, airway management, perioperative complications, and causes of death were identified. IRB approval was obtained.
Results: Nine of the 12 patients required a total of 49 anesthetics for 81 different procedures (1 - 16 anesthetics per patient). All patients were classified as ASA 4. There were ten serious perioperative complications, most often difficult intubation requiring three or more attempts, fiberoptic intubation or tracheostomy (n=4). All of these patients had a preoperative diagnosis of “abnormal airway†such as micrognathia and limited mouth opening. Cardiopulmonary arrest occurred in 2 patients, and emergent intubation outside the operating room was required in 3 patients. There were an additional 28 cases of difficult mask ventilation or multiple intubation attempts. In multiple patients the LMA or Glidescope were too large to fit the patient’s small mouth opening, and there was difficulty with fiberoptic intubation due to poor visualization.
Discussion: Our review of Trisomy 18 patients at Children’s Hospital of Wisconsin shows that most patients have comorbid conditions that affect anesthetic management. We demonstrate that these patients are at high risk for perioperative complications, especially airway complications. The anesthesiologist must anticipate a difficult airway in all of these patients, and the preoperative exam is often predictive. Our review also highlights that Trisomy 18 patients can undergo a multitude of procedures requiring anesthesia. Considering that 90% of Trisomy 18 patients die by 12 months of age (2), the necessity of each procedure and the high associated risk must be weighed against the potential benefits. To date, many of these patients continue to be “full code†at our institution. Clear communication of the anesthetic risks and collaboration with the family and care team are vital.
Conclusion: We demonstrate that patients with Trisomy 18 are at high risk for perioperative complications, especially complications involving airway management.
References:
1. Courreges P., et al. (2003) Paediatric Anaesthesia 13: 267-269.
2. Imataka, G., et al. Molecular Medicine Reports 13.3 (2016): 2457-2466.
-
 NM-206 Image 1
NM-206 Image 1
Top










