
NM-196
When Best-Laid Plans Go Awry: Successful Nasal Intubation in a Developmentally Delayed Teenager with Jaw Fracture Despite Equipment Failure and Copious Nasal Bleeding
Eklund J, Jones L
University of Illinois Medical Center, Chicago, IL, UIC
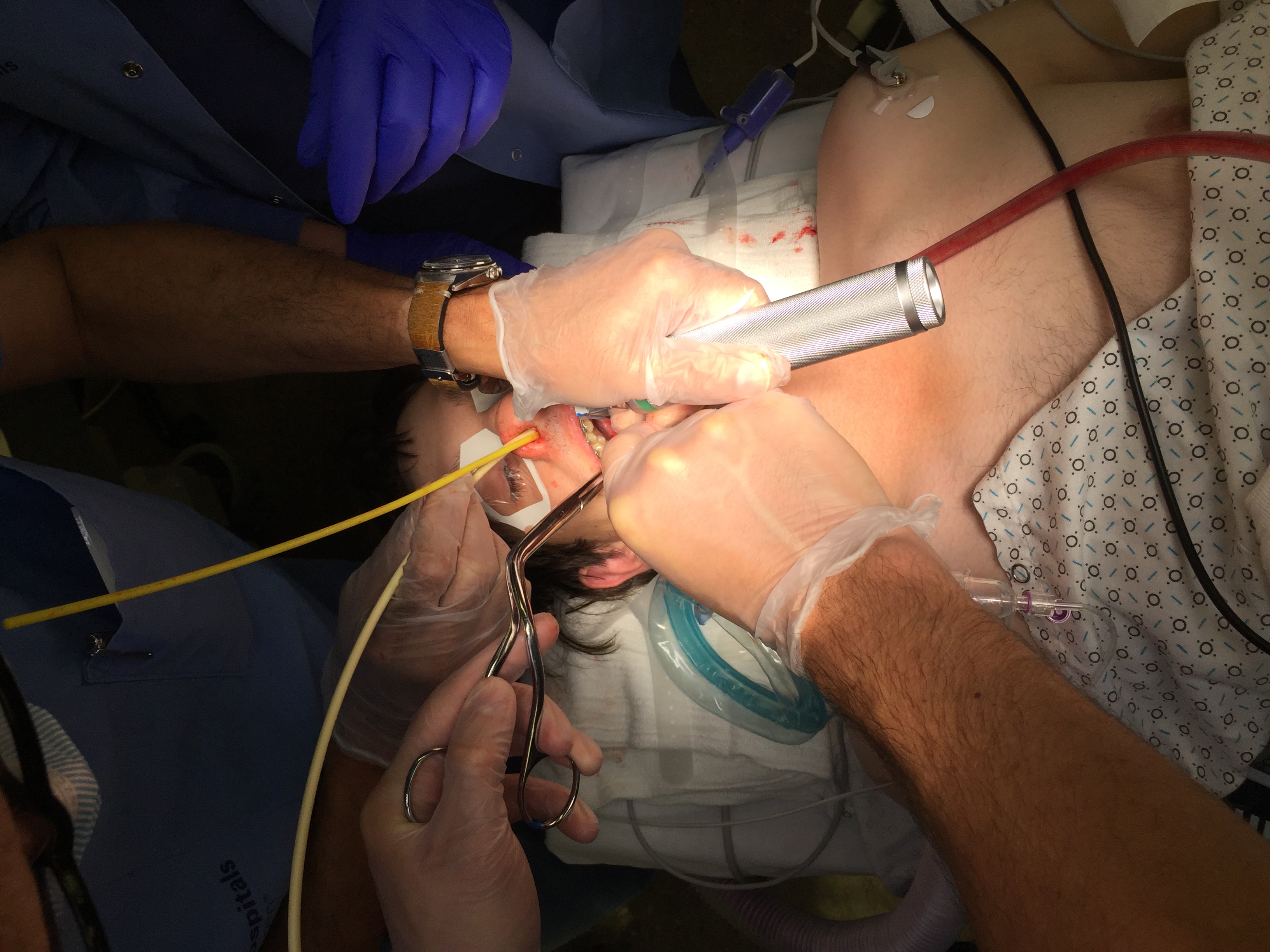
An 18 y/o developmentally-delayed, obese boy with anxiety and polysubstance abuse history presented for ORIF left mandible. Exam findings included: mouth opening limited by pain with unknown Mallampati score, wide neck girth, and 5-FB TMD. The Oral-Maxillofacial Surgery service requested nasal intubation. Awake nasal fiberoptic intubation (FOI) was deferred due the patient’s anxiety and lack of cooperation. The initial plan was asleep nasal intubation via direct laryngoscopy (DL). All equipment was tested during room set-up. A videolaryngoscope (VL) and supraglottic airway (SGA) were immediately available.
After induction, the nares were topicalized with oxymetazoline and serially dilated with lubricated nasal trumpets. Profuse nasal bleeding pooled as the softened nasal RAE ETT was advanced into a nare. DL proceeded with Gr. 1 view, but the laryngoscope’s light bulb failed. VL was immediately initiated, but the disposable cover fogged up. A nasal trumpet with oxymetazoline was inserted to tamponade the bleeding. Using the VL to perform DL, oral intubation was achieved. The SpO2 raised to 100%. Discussion with OMFS team concluded that nasal intubation was still necessary.
After suctioning the nares, an airway-exchange catheter (AEC) was passed blindly through the nasal trumpet into the hypopharynx. Using a new disposable VL cover, the AEC passed through the cords alongside the oral ETT. Using the Seldinger technique, a new nasal ETT was advanced to the glottis. Next, the oral ETT was removed so that the nasal ETT could advance through the cords. Surgery proceeded without issues. The nasal ETT tamponaded bleeding, and the patient was uneventfully extubated.
Airway management of developmentally-delayed adolescent patients with oral maxillofacial injuries is challenging, especially when compounded by the surgical requirement for nasal intubation. Previous case reports of using bi-orifice intubation and Seldinger technique with bougie or airway catheter have been published [1,2,3,]. While asleep nasal FOI may have seemed appropriate initially, it likely would have also resulted in bleeding. Likewise, using a “red-rubber†catheter to blunt nasal trauma or a gum-elastic bougie with Seldinger technique initially may have reduced the likelihood of nasal trauma.
This case highlights the utility of the bi-orifice approach as a Plan C to quickly secure an airway and subsequently avoid the “emergent†branch of the Difficult Airway Algorithm. Advantages to this approach include: uninterrupted ventilation and oxygenation, reduced risk of airway loss, ability to administer non-depolarizing muscle relaxant, and time to discuss an alternate plan with surgical colleagues [3].
Abrons RO et al. Anaesthesia. 2017 Sep 15.
Abrons RO et al. J Clin Anesth. 2016 Nov;34:609-11.
Eklund JE et al. J Clin Anesth 2017; 43: 68-69.
-
 NM-196 Image 1
NM-196 Image 1
Top










