
NM-368
Fetoscopic Myelomeningocele Repair: Fetal Wellbeing & Mode of Delivery
Sutton C, Kim J, Aina T, Chandrakantan A, Hassanpour A, G D, Patino M, Olutoye O, Belfort M, Shamshirsaz A, Espinoza J, Whitehead W, Olutoye O
Texas Children's Hospital, Houston, Texas, USA
Intro:
Myelomeningocele (MMC) is the most common congenital anomaly of the central nervous system that is compatible with life. Despite early postnatal repair, patients with MMC often have permanent disability. Evidence now supports the safety and efficacy of prenatal repair(1), but fetal intervention entails maternal risk that is not present with postnatal repair, including the serious risk of uterine scar dehiscence following open fetal repair.(2)
Minimally invasive fetoscopic MMC repair allows for the possibility of vaginal delivery, but the impact of carbon dioxide (CO2) insufflation on fetal wellbeing is poorly understood. We performed a retrospective chart review with a primary aim of determining ultimate mode of delivery after fetoscopic MMC repair, and a secondary aim of evaluating whether intra-amniotic insufflation of CO2 impacts fetal wellbeing during fetoscopic MMC repair.
Methods:
Retrospective chart review of all patients with MMC scheduled for fetoscopic repair from June 2015-June 2017 was performed. Baseline patient demographics, surgical, and obstetric outcomes were collected.
We also collected intraoperative arterial blood gas results and fetal heart rate (FHR) during the procedures. To understand how the duration of CO2 insufflation impacted fetal wellbeing, we used a mixed-effects model using FHR at 0, 30, 60, and 120 minutes after insufflation.
Results:
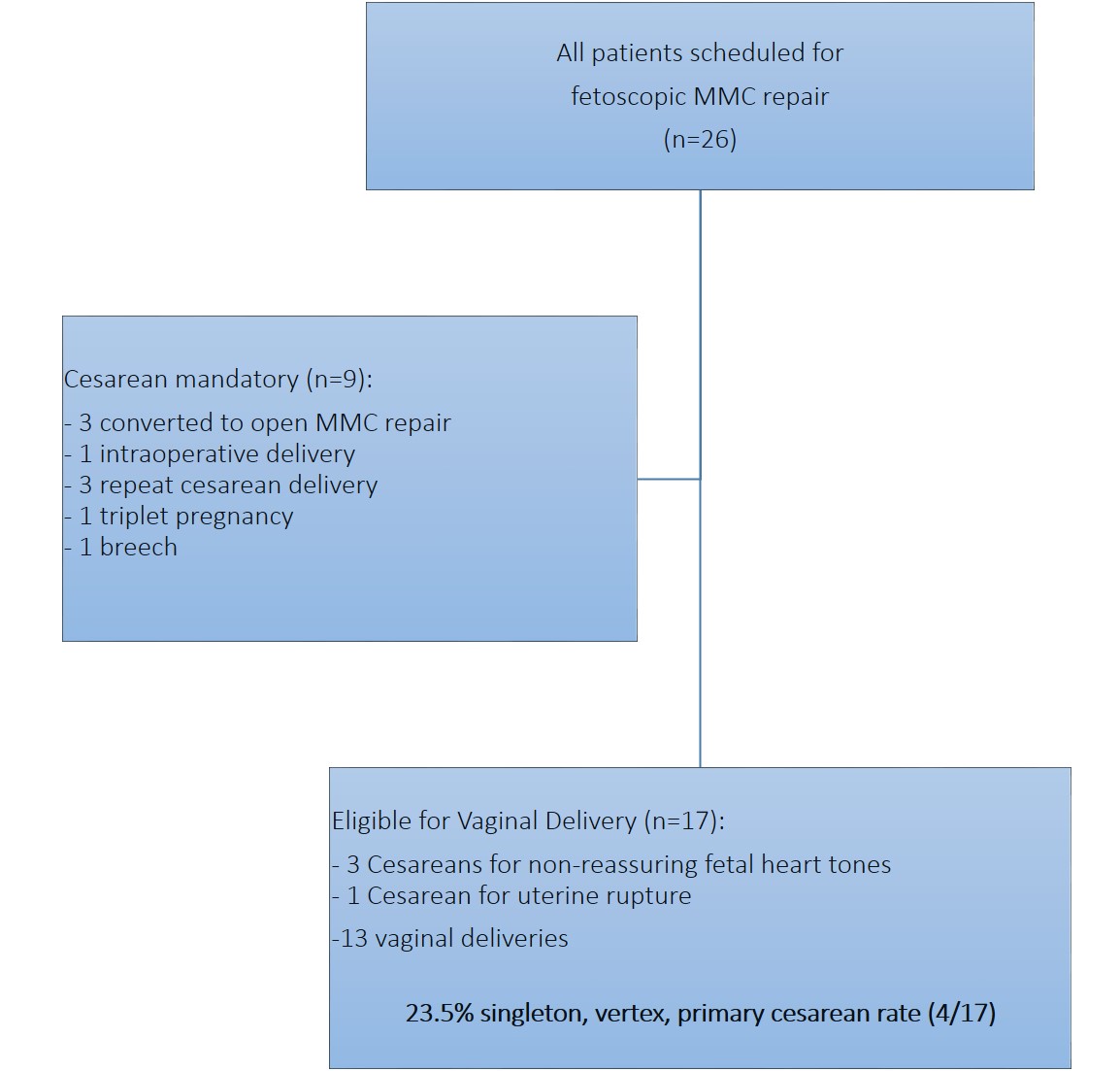
26 patients were scheduled for fetoscopic MMC repair during the study period. Obstetric outcomes are shown in Fig 1. The singleton, vertex, primary cesarean rate was 23.5%.
For our secondary outcome, FHR data was not recorded in 2 cases, and the 3 cases converted to open repairs were excluded. The remaining 21 cases were considered in the mixed effects model. Duration of intra-amniotic CO2 insufflation did not significantly affect FHR over time (SE=-0.54, 95% CI -1.62 to 0.55, p=0.33).
Discussion:
Fetoscopic MMC repair offers the potential benefit of decreased maternal morbidity by allowing for the possibility of a vaginal delivery. Our center’s experience showed a singleton, vertex, primary cesarean rate of 23.5%, well below the 100% cesarean rate mandated by open prenatal MMC repairs.
FHR was not impacted by the duration of CO2 insufflation, demonstrating that fetal distress does not appear to be associated with length of intra-amniotic CO2 insufflation.
Conclusion:
The potential decrease in maternal morbidity and the lack of evidence of intra-operative fetal distress despite lengthy intra-amniotic CO2 insufflation warrants continued evaluation of fetoscopic repair techniques.
1. Adzick S, et al. A Randomized Trial of Prenatal versus Postnatal Repair of Myelomeningocele. NEJM, 2011.
2. Johnson M, et al. The Management of Myelomeningocele Study: obstetrical outcomes and risk factors for obstetrical complications following prenatal surgery. AJOG, 2016.
-
 NM-368 Image 1
NM-368 Image 1
Top










