
NM-353
Combination of Demand Only PCA and Short Term Methadone to Decrease Length of Stay in Sickle Cell Disease Vaso-occlusive Acute Pain
1Liebling D, 1Manwani D, 1Carullo V, 2Choi J, 2Gao Q, 3Moody K
1Montefiore Medical Center, Bronx, NY, United states; 2Albert Einstein College of Medicine, Bronx, NY, United states; 3University of Texas MD Anderson Cancer Center, Houston, TX, United states
Introduction: Sickle cell disease (SCD) is a chronic illness characterized by unpredictable episodes of pain and high-health care utilization rates. There is controversy regarding the method of administration of opioids via PCA, with studies examining varying ratios of continuous to demand dosing. PCA with basal infusion plus demand dosing seems to be preferred by the hematology community whereas emerging data in other populations demonstrate adequate pain control and reduced rates of opioid-related adverse events with the use of demand only approaches. In October 2012, as part of a quality improvement initiative at the Children's Hospital at Montefiore, we revised our pain management guidelines to exclude the routine use of basal infusions in our PCA protocol. Short-term methadone during the inpatient stay with a short taper post discharge was utilized for improved acute pain control and long-acting analgesia in patients that did not improve rapidly on the standard regimen.
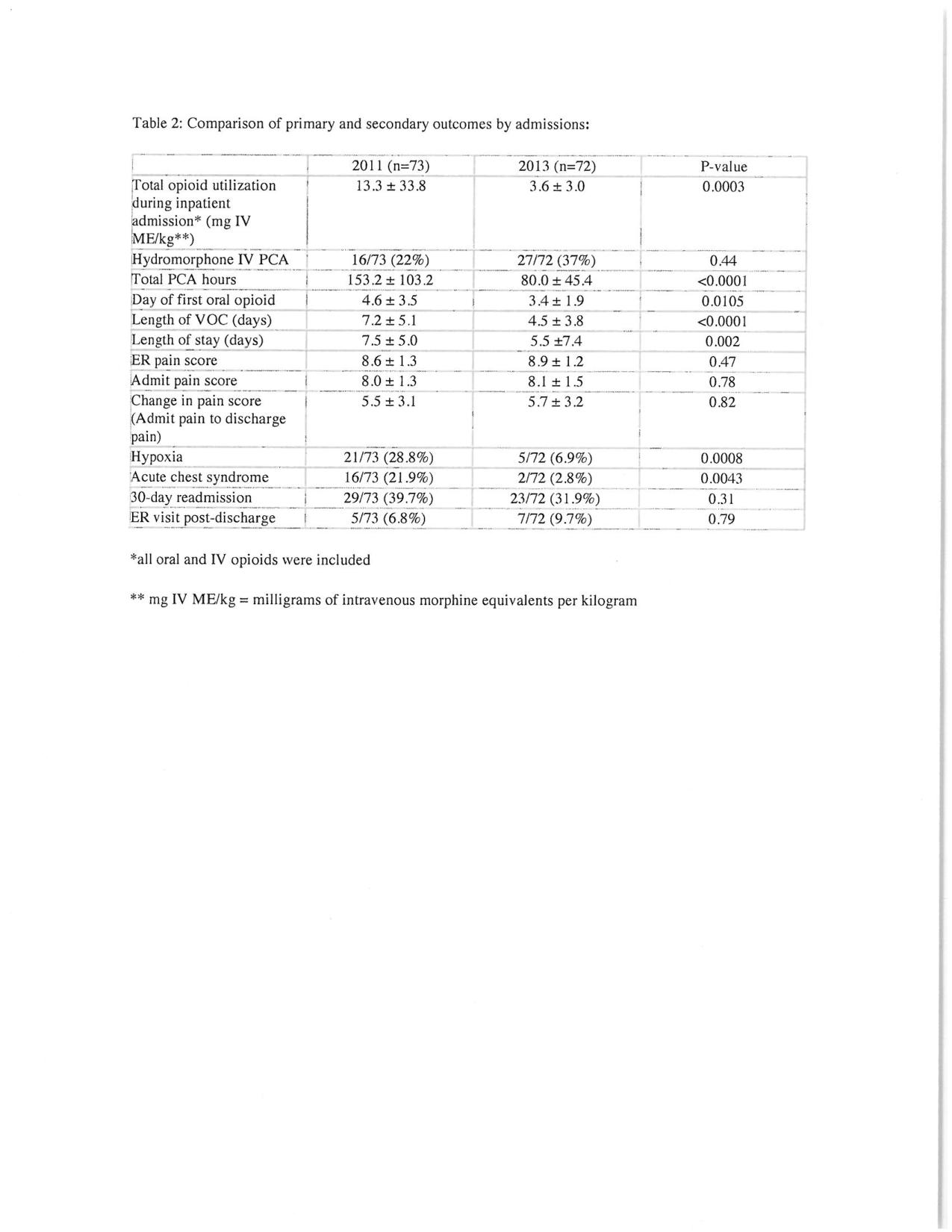
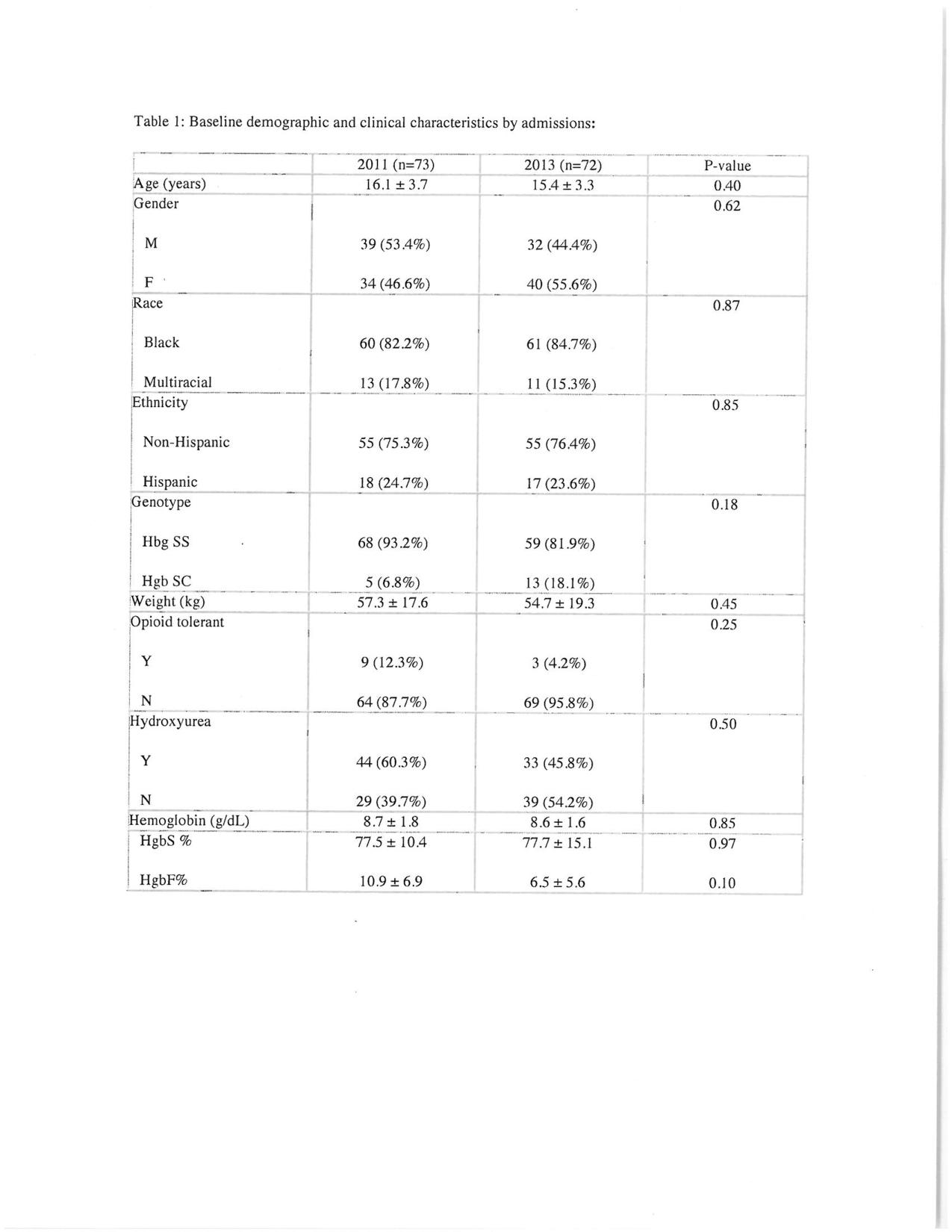
Methods: We conducted a retrospective analysis of patients with SCD < 21 years of age, admitted for VOC 3-7 times/year, comparing patient admissions in 2011 versus 2013, pre- and post-revision of the pain protocol as described above. Primary outcomes include total opioid utilization during inpatient admission, total hours on intravenous PCA and length of stay (LOS).
Results: A total of 144 admissions were included in the analysis, 73 in 2011 and 72 in 2013. In 2011, 72/73 patient admissions were treated with PCA with basal infusion compared to only 1/72 patient in 2013. Seven out of 73 admissions in 2 patients in 2011 required the use of methadone compared to 9 admissions out of 73 in 4 patients in 2013. In 2011, methadone was used in patients that were opioid-tolerant for the management of chronic pain. In 2013, methadone was used for the management of intractable acute pain unresponsive to intravenous short-acting opioids with PCA. Total opioid utilization during inpatient admission, total PCA hours and LOS were significantly reduced in the 2013 group compared to the 2011 group (Table 2). Furthermore, patients in the 2013 group demonstrated a significantly lower incidence in episodes of hypoxia and acute chest syndrome (Table 2)
Conclusions: In conclusion, we demonstrate the feasibility and benefits of demand only PCA in the management of VOC pain. In the small number of patients who experience intractable pain unresponsive to IV PCA, methadone can provide acute pain control and can help facilitate transition from intravenous patient-controlled analgesia to an oral opioid regimen.
-
 NM-353 Image 2
NM-353 Image 2 -
 NM-353 Image 1
NM-353 Image 1
Top










