
OS2-147
Perioperative outcomes and management comparing high surgical volume vs. low surgical volume centers for complex cranial vault reconstruction: a multicenter study from the Pediatric Craniofacial Collaborative Group
1Fernandez A, 2Reddy S, 2Gordish-Dressman H, 3Muldowney , 4Martinez J, 5Chiao F, 6Stricker P
1Johns Hopkins All Children's Hospital, St Petersburg, FL, USA; 2Children's National Medical Center, Washington DC, Washington, USA; 3University of Wisconsin-Madison, Madison, WI, USA; 4Université de Montréal, Montréal, QC, Canada; 5Weill Cornell Medical College, New York, New york, USA; 6Childrens Hospital of Philidelphia, Philadelphia, PA, USA
Introduction: Surgical correction of craniosynostosis is a complex procedure in infants and children that results in significant blood loss. The most severe and most common perioperative issues relate to the rate and extent of blood loss. As complex cranial vault reconstruction (CCVR) is an infrequent procedure, no information is available to compare blood transfusion rates and related consequences between high volume institutions and low volume institutions. Thus, the aim of this study was to determine blood donor exposure variability among institutions based on CCVR surgical volume. We hypothesized that there is no relationship between CCVR case volume and total perioperative blood donor exposures.
Methods: Infants and children with craniosynostosis undergoing CCVR between June 2012 and September 2016 as part of the Pediatric Craniofacial Surgery Perioperative Registry (PCSPR) were retrospectively evaluated. Institutions contributing data to the PCSPR were categorized as low, middle, and high volume centers, based on their average number of CCVR cases per month. The primary outcome measure was total blood donor exposures, while secondary outcome measures included operative time, volume of blood transfusion, ICU and hospital length of stay, and incidence of major perioperative complications. Normality of all continuous outcomes was determined and means were compared using ANOVA for normally distributed variables and Kruskal-Wallis non-parametric test for non-normally distributed variables. Categorical outcomes were compared using a chi-squared test. A p-value of <0.05 was considered statistically significant.
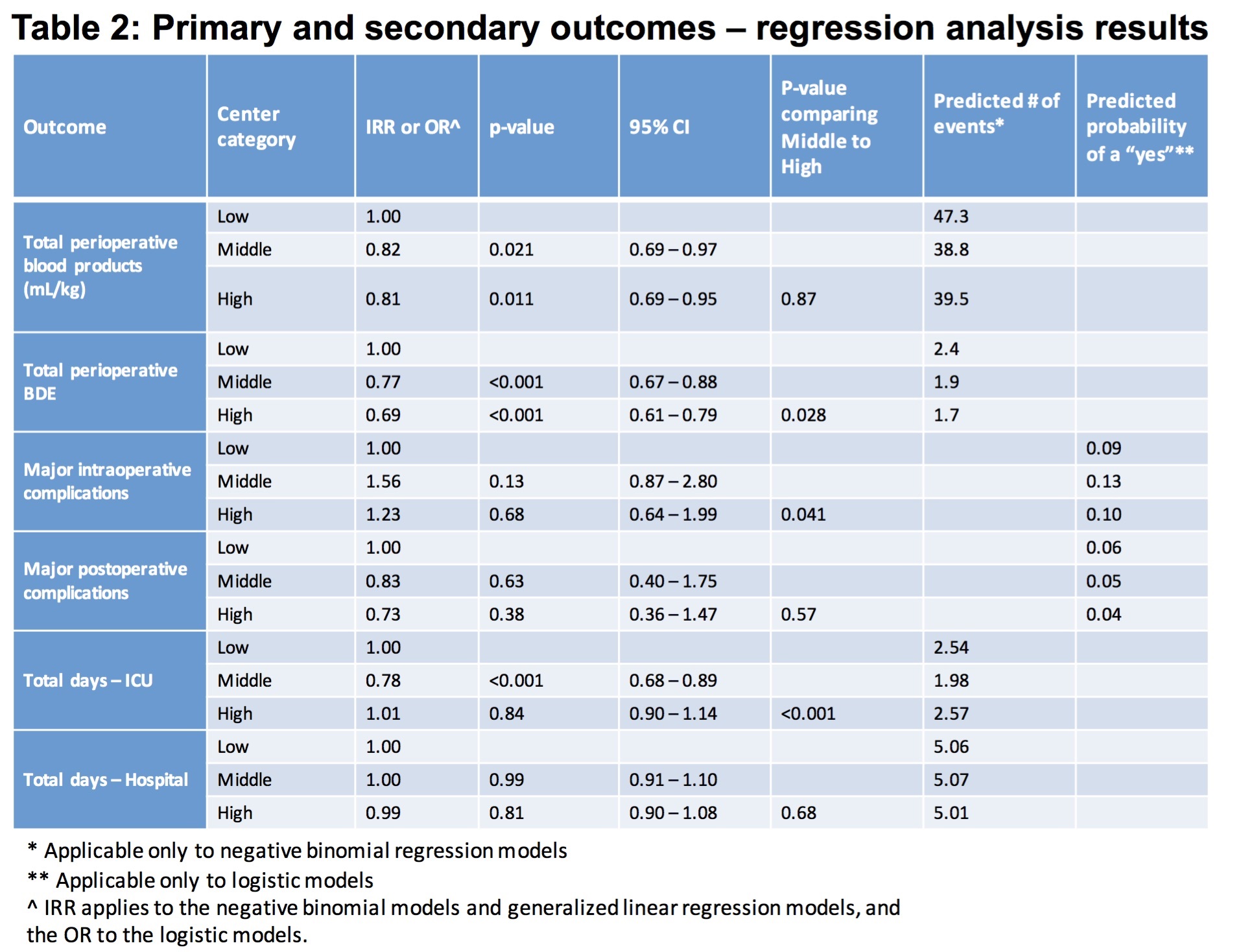
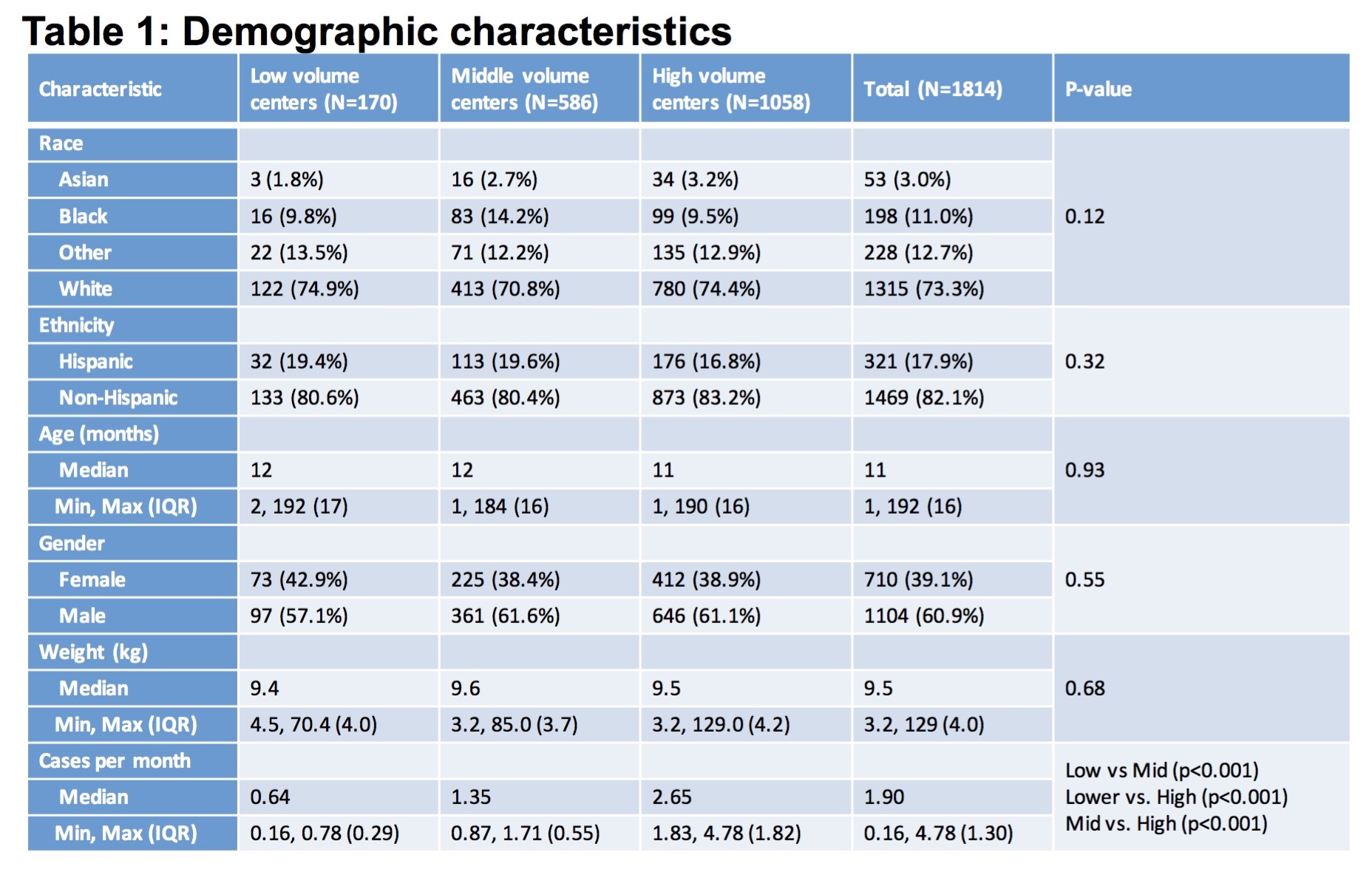
Results: Thirty-three institutions contributed data to the PCSPR during the study period which included a total of 1814 CCVR cases. There were no significant differences in demographics or operative times between high, middle, and low volume centers (Table 1). However, high volume centers had significantly fewer blood donor exposures than both middle and low volume centers. High and middle volume centers had less blood transfusion volumes (in mL/kg) than low volume centers. High volume centers also had significantly fewer intraoperative complications than middle volume centers. In addition, middle volume centers had lower ICU length of stays than both high and low volume centers, while there were no differences in total hospital length of stays or postoperative complications observed between the three groups (Table 2).
Conclusion: Infants and children who undergo CCVR at high surgical volume centers are associated with fewer blood donor exposures and transfusion volumes (in mL/kg) than lower volume centers.
-
 OS2-147 Image 2
OS2-147 Image 2 -
 OS2-147 Image 1
OS2-147 Image 1
Top










