
NM-301
The Effect of Hypothermia on Transfusion Requirement During and Immediately After Pediatric Craniofacial Surgery: A Retrospective Study.
Fuller H, Fiedorick C, Poteet-Schwartz K, Apuya J
University of Arkansas Medical Sciences/Arkansas Children's Hospital, Little Rock, Arkansas, USA
Introduction: The primary anesthetic consideration in the management of children undergoing craniofacial surgery is intra-operative hemorrhage. According to the Pediatric Craniofacial collaborative group, majority of these patients receive blood transfusion.1 We identified only one retrospective risk factor analysis for blood loss during pediatric craniofacial surgery in which there was no association found between intra-operative hypothermia and increased blood loss.2
We hypothesize that there is an association between hypothermia (<35.5 °C) and intraoperative blood transfusion requirements in craniofacial surgery.
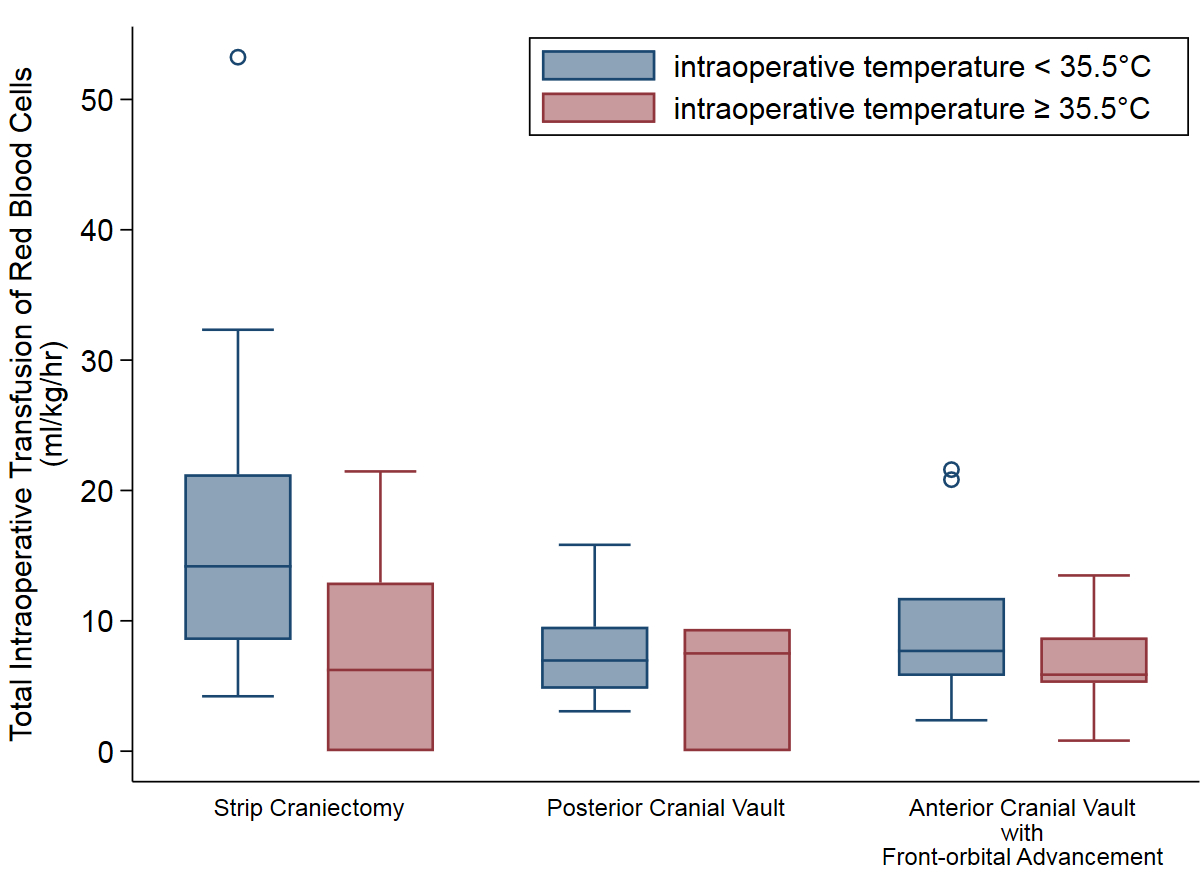
Methods: After IRB approval was obtained, a retrospective analysis was done which included 86 patients undergoing craniofacial surgery our institution. Demographics analyzed included: patient age, gender, weight and craniosynostosis diagnosis. Surgical factors analyzed included: total operative time and the following surgical procedure type: strip craniectomy, anterior cranial vault/fronto-orbital advancement, or posterior cranial vault. Primary outcome data was total intraoperative blood transfusion and the secondary outcomes included: total intraoperative fluid administration postoperative blood transfusions within twenty-four hours of the procedure.
Results: There were 48 patients in the hypothermic group (intraoperative temperature nadir <35.5 °C) and 38 patients in the normothermic group (≥35.5°C). A statistically significant association exists between intraoperative hypothermia and intraoperative transfusion of red blood cells. Analysis showed 6.03 ml/kg/hr greater intraoperative transfusion requirement between the two groups (P=<0.001). To account for fluid administration (FA), two groups were created: low (≤20ml/kg/hr) and high (>20ml/kg/hr). A 34% increase in intraoperative red blood cell transfusion requirement in the hypothermic (<35.5 °C) group compared to the normothermic (≥35.5°C) group for low FA. When FA was ≥20ml/kg/hr, the transfusion requirement increased to 51% (P=<0.001).
Discussion: In this study, an association between intraoperative hypothermia and increased intraoperative transfusion of red blood cells. The difference between the groups was a clinically significant amount of 6.03ml/kg/hr. This finding corresponds with known associations between hypothermia and coagulopathy, and between blood loss and intraoperative hypothermia in various types of surgery in adults.
Conclusion: Careful management of temperature ≥35.5 °C reduces intraoperative transfusion requirements and possibly its significant associated morbidities in this patient population.
References:
1. Sticker, PA, et al. Anesthesiology 2017;126(2):276-287.
2. Gonzalez-Cardenas, VH, et al. Rev. Colomb. Anesthesiol. Vol 44(3) Bogota July/Sep. 2016.
-
 NM-301 Image 1
NM-301 Image 1
Top










