
NM-229
Pediatric Critical Airway Team (P-CAT): Problem Identification, Needs Assessment and Implementation
Kriss R
UC Davis Children's Hospital, Sacramento, CA, US
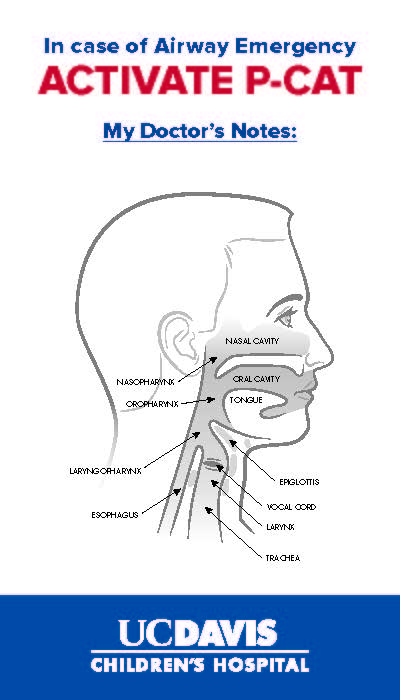
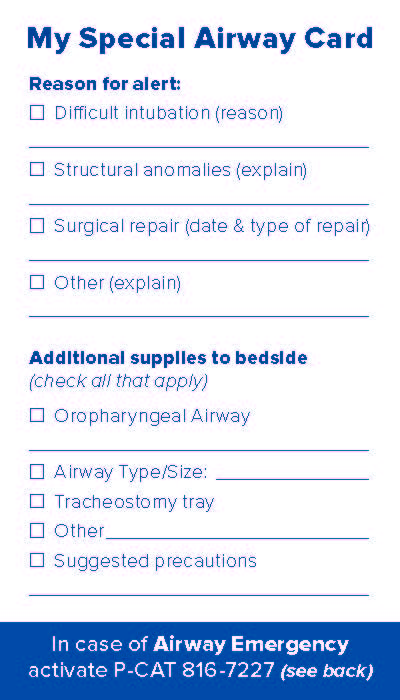
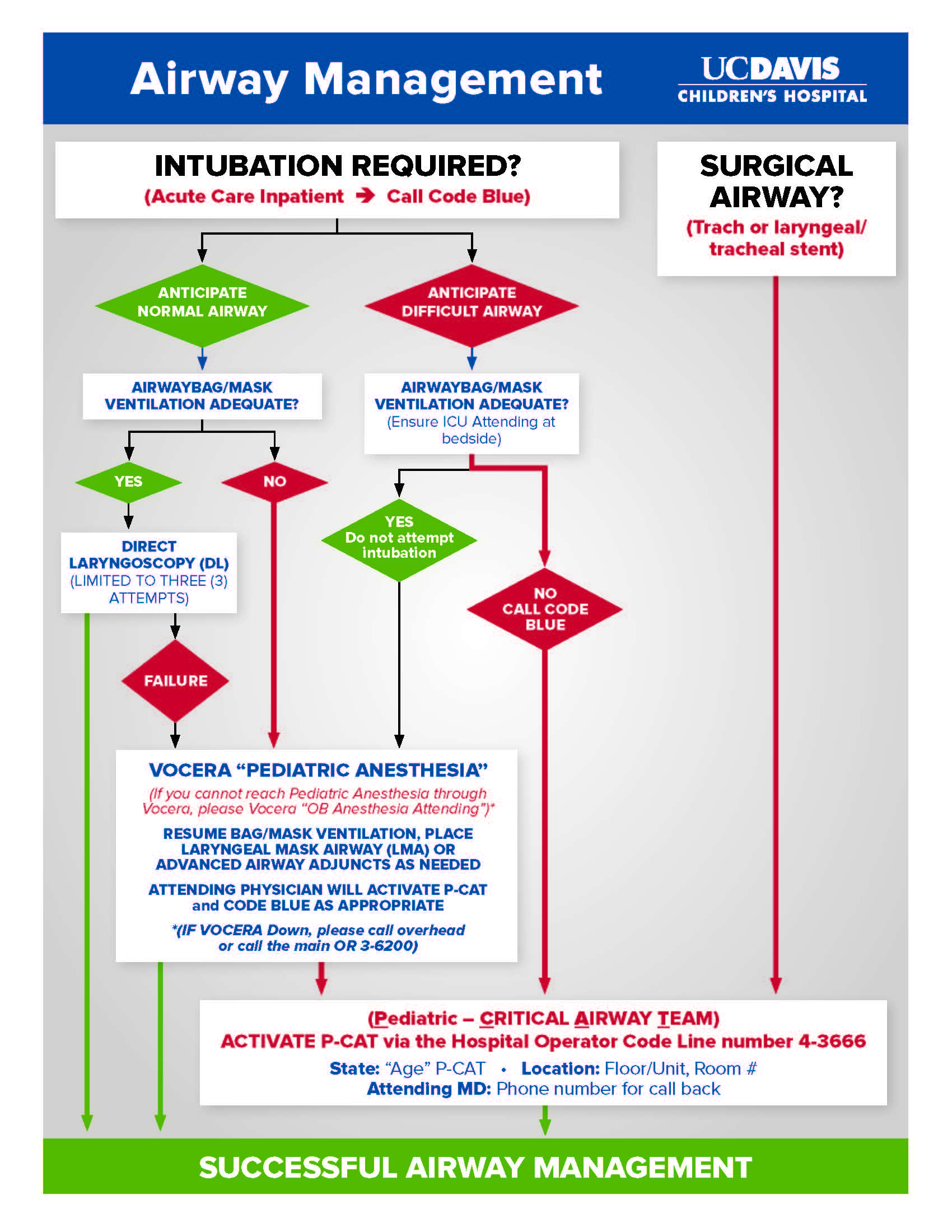
Introduction: UC Davis Children’s Hospital is an ACS Level 1 Hospital contained within the adult Medical Center. Four (4) significant near-miss pediatric airway events prompted the need for a specialized, multi-disciplinary Pediatric Attending team to be on-call for immediate response to these life-threatening yet low frequency events. Multiple responders, multiple intubation attempts, scattered equipment, and lack of coordinated effort were identified issues limiting optimal outcomes. A team from Anesthesiology, ENT, Pediatric Surgery, Trauma Surgery, Emergency Department and Critical Care met and determined that standardizing our process will improve outcomes. The Acute Airway Teams developed at other children’s hospitals were base models; however, many significant modifications were made since our non-free standing children’s hospital has most pediatric specialists on call from home. Initially, in-house call attendings were identified as Pediatric ICU, ED, OB Anesthesiology and Trauma Surgery as well as essential pediatric specialists that were not in-hospital, Pediatric Anesthesiology, ENT and Pediatric Surgery. An algorithm was developed to include all pediatric patient locations, patient ages and utilizing in-house attendings where possible, to triage and make essential airway interventions until the P-CAT team has arrived. The recognized delay in identifying known pediatric difficult airways (multiple identification systems were already in place) was replaced with a standardized, single Difficult Airway bedside card, including written and graphic description of the airway, and would now accompany all difficult airway patients during their entire hospitalization.
It was also determined that a comprehensive, standardized cart would be essential including all Anesthesiology and Surgical emergency airway equipment. The cart would be housed in the Pediatric ICU and maintained by respiratory therapy and have interchangeable OR trays for quick, sterile replacement of surgical equipment. The cart contents were very broad to include the needs of multiple surgical services (Pediatric surgery vs. ENT), highly variable locations (including ICUs, floor and ED) and the diverse patient population from neonate to teenager.
The P-CAT team currently responds to all pediatric critical airway events throughout the Children’s Hospital and has successfully managed many situations in its less than 6 month existence.
Conclusion: The Pediatric Critical Airway Team (P-CAT) at UC Davis Children’s Hospital demonstrates that the approach utilized at many stand alone Children’s Hospitals can be successfully adapted and implemented at a non-free standing children’s hospitals if novel modifications are applied to include initial triage and preparation by existing in-house resources allowing pediatric specialists to arrive.
-
 NM-229 Image 3
NM-229 Image 3 -
 NM-229 Image 2
NM-229 Image 2 -
 NM-229 Image 1
NM-229 Image 1
Top










