
NM-343
How Not to do Anesthesia: Decreasing Pediatric Exposure to Anesthesia for MRI
Lammers C, Andalis, ccls C, Wetzel S
UC Davis Children's Hospital, Sacramento, CA, USA
As research studies continue to accumulate associations between exposure to anesthesia and cognitive dysfunction/learning and behavioral diagnoses in children1, anesthesiologists are motivated to minimize these exposures. Anesthesiologists provide many hours of anesthesia to pediatric patients for radiologic exams. Combined MRI studies can take up to 3 hours, and many patients come for repeated studies as frequent as every 3 months. Historically, as pediatric anesthesiologists we encouraged families to attempt diagnostic scans without anesthesia but this was time consuming and had limited success. This led to lost anesthesiology service time while on “standby†and lost revenue for radiology because there was no structure to the “attemptsâ€. Lost revenue for an unused MRI scanner is approximated at $500 per hour.
We teamed together with the Departments of Radiology and Child Life to provide a collaborative and successful approach to scheduling and obtaining MRI exams without anesthesia.
We expanded the guidelines for schedulers to identify children that were good candidates to avoid anesthesia. For children that were uncertain or close to age cutoffs, we offered early non-anesthesia AM slots that were just prior to an anesthesia “add-on†slot as a backup plan. The child life department dedicated a child life specialist one day per week for MRI scans without anesthesia. A Children’s Miracle Network grant provided the funds to purchase MRI compatible movie goggles.
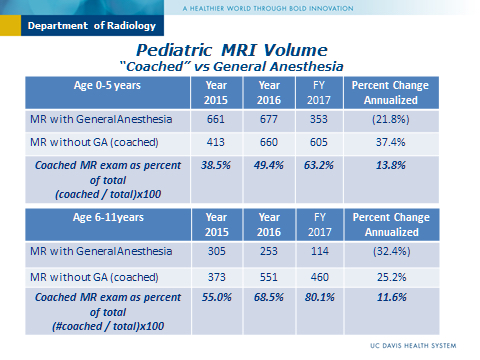
In our case series, children 6 to 11yo had an 80% success rate and children 0-5yo had a 63% success rate for obtaining MRI exams without anesthesia. This was a significant improvement compared to the prior years. Importantly, the child life specialist’s involvement helped educate the MRI technologists and families and change the culture of how radiology exams are obtained.
The FDA MedWatch released in December 2017 warned that “Health care professionals should balance the benefits of appropriate anesthesia in young children and pregnant women against the potential risks, especially for procedures that may last longer than 3 hours or if multiple procedures are required in children under 3 years.â€2 It is our responsibility as pediatric consultants to identify opportunities to decrease or avoid anesthesia in children.
What started out as a struggle to balance a pediatric anesthesiologist’s objective to minimize anesthesia exposure with lost anesthesiology service time and revenue led to a highly successful team approach.
1Jevtovic-Todorovic, Vesna. “Anesthetics and Cognitive Impairments in Developing Children.â€JAMA Pediatrics, 2 Oct. 2017, doi:10.1001/jamapediatrics.2017.3033.
2“Safety Alerts for Human Medical Products - General Anesthetic and Sedation Drugs: Drug Safety Communication - New Warnings for Young Children and Pregnant Women.†U S Food and Drug Administration Home Page, Office of the Commissioner, 14 Dec. 2016.
-
 NM-343 Image 1
NM-343 Image 1
Top










