
NM-232
Awake Caudal in Young Infants Using Chloroprocaine as the Sole Anesthetic: A Retrospective Review
1Ramsey M, 2Ta J, 1Hajduk J, 1Wieser J, 1Jagannathan N, 1Suresh S
1Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, US; 2Rush University Medical Center, Chicago, IL, US
Background:
When used as the sole anesthetic technique, awake caudals offer advantages of reducing opioid and volatile agent requirements. Chloroprocaine is a local anesthetic with rapid action onset/offset and short half-life, making it a viable alternative for use in neonates and infants undergoing short duration procedures. Dosing recommendations for chloroprocaine caudal blocks are poorly established with infusion ranges from 6.75 to 45mg/kg/hr (1, 2) and 30mg/kg bolus with 30mg/kg/hr infusion (3). Currently, there is a paucity in dosing, safety, and efficacy data of awake single injection caudal blocks. We therefore present our institutional experience with this technique in infants undergoing lower extremity procedures.
Methods:
Following IRB approval, medical records of infants who received single-shot caudal anesthesia with chloroprocaine for tendo-achilles lengthening were reviewed. Surgical duration, chloroprocaine dosage, complications, and postoperative pain scores were abstracted. The primary outcome was the efficacy of caudal blockade.
Results:
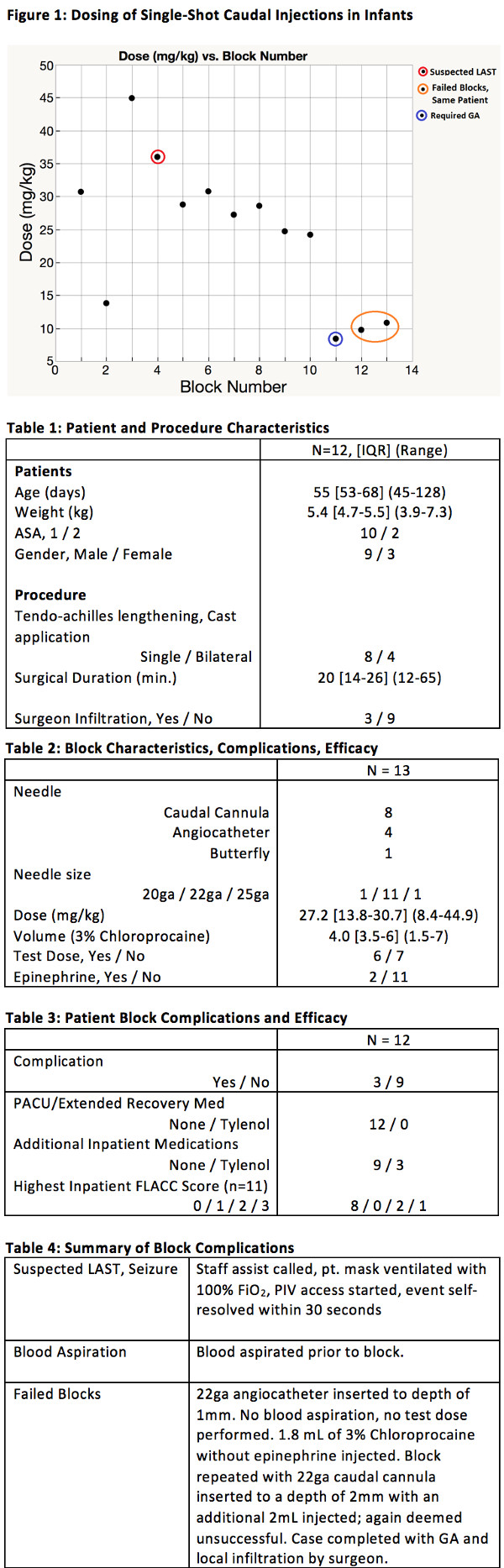
Twelve infants were included in the analysis. In 11 patients, a rapid onset of motor and sensory block in the lower extremities and provided adequate operating conditions. A seizure due to LAST was the major complication in one infant, and failed block requiring GA in another. Dosing regimens varied and ranged from 8.4 mg/kg to 44.9 mg/kg. In the case of failed neuraxial technique requiring conversion to GA, a lower dose of 9.75 mg/kg was used. In the case of suspected LAST, a higher dose of 36 mg/kg was used. Postoperatively, all patients had a pain score of 0 at the time they were discharged from Phase 1 recovery. No patients required additional medications for analgesia immediately postoperatively.
Discussion:
A range of doses provided rapid onset of motor and sensory block, with toxicity and failed block occurring at the upper and lower ranges, respectively. A dose of 30 mg/kg of 3% Chloroprocaine is likely a safe and effective dose in providing adequate regional anesthesia to patients undergoing lower extremity surgeries of duration up to 30 minutes. Future up and down dosing studies should be conducted to determine the lowest dosage resulting in effective anesthesia.
Conclusion
Awake caudal anesthesia with chloroprocaine, with appropriate dosing, can be used as the sole anesthetic in shorter surgical procedures of the lower extremities.
References:
1. Muhly WT. A retrospective comparison of ropivacaine and 2-chloroprocaine continuous thoracic epidural analgesia for management of postthoracotomy pain in infants. Paediatr Anaesth. 2015 Nov;25(11):1162-7.
2. Tobias JD. Chloroprocaine for epidural anesthesia in infants and children. AANA J. 1995 Apr;63(2):131-5.
3. Henderson K. Continuous caudal anesthesia for inguinal hernia repair in former preterm infants. J Clin Anesth. 1993 Mar-Apr:5(2):129-133.
-
 NM-232 Image 1
NM-232 Image 1
Top










