
GAP-106
Williams Syndrome: A Day in the Dental Room
Zapata A, Motta P
Texas Children's Hospital, Houston, TX, USA
As a pediatric anesthesiologist some of the most difficult patients to manage are children with Williams syndrome (WS). The most concerning aspect of their care is the risk of peri-procedural cardiac arrest. We will discuss the anesthetic management of a patient with WS undergoing dental extraction.
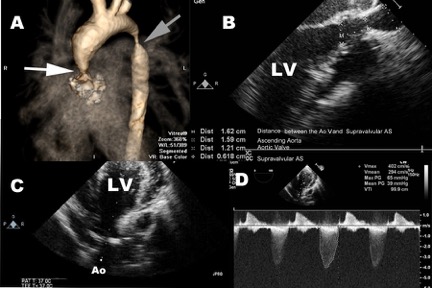
A 7yo 23 kg M with WS, severe supravalvar aortic stenosis (SVAS) (Fig 1), left ventricular hypertrophy, stenotic RCA, dilated LAD, severe coarctation, and asthma presents for dental extraction prior to cardiac surgery. He was pre-medicated with 2mg intravenous (IV) midazolam and taken to the OR. After application of ASA monitors, the patient underwent controlled induction with lidocaine, midazolam, titrated fentanyl (1mcg/kg x2), etomidate, rocuronium, 1% sevoflurane and intermittent phenylephrine boluses to maintain pre-operative blood pressures. He was then orally intubated and a radial arterial line was placed. Due to ST changes with minimal hypotension while using low inhaled anesthetic doses, the patient was started on a low dose vasopressin infusion to maintain mean arterial pressures within 10 percent of baseline. During the dental extraction, he had multiple episodes of tachycardia with associated hypotension which required treatment with esmolol. He was reversed with a titrated glycopyrrolate dose to prevent excessive tachycardia and extubated deep on dexmedetomidine. He was then admitted to ICU for monitoring while awaiting his cardiac surgery.
The incidence of WS is approximately 1 in 10,000 - 20,000 live births. Due to their multisystemic illness, they tend to have several procedures requiring either sedation or general anesthesia in their lifetime. The underlying genetic abnormality is a deletion on chromosome 7q11.23 which leads to a defect in the elastin gene and subsequently the elastic structure of vascular walls. They may present with SVAS, supravalvar pulmonary stenosis, peripheral pulmonary artery stenosis, coronary anomalies, prolonged QT, developmental delay and difficult airways. As anesthesiologists we should always consider invasive monitoring, be prepared for cardiac arrest, and the need for emergent circulatory support. Due to the potential risk of severe complications these patients need to be done in a tertiary center and never as outpatients. Intra-operative goals should include maintenance of pre-operative blood pressures, NSR, avoiding tachycardia, maintaining preload and SVR, and prevention of elevated PVR.
References
Collins RT, et al. Peri-procedural risk stratification and management of patients with Williams syndrome. Congenital Heart Disease. 2017;12:133–142.
Burch, T. M., et al. (2008). Congenital supravalvular aortic stenosis and sudden death associated with anesthesia: What's the mystery? Anesthesia & Analgesia, 107(6), 1848-1854.
Matisoff AJ, et al. Risk assessment and anesthetic management of patients with Williams syndrome: a comprehensive review. Paediatr Anaesth. 2015;25(12):1207–15.
-
 GAP-106 Image 1
GAP-106 Image 1
Top










