
GA1-48
Portal Vein and Hepatic Artery Thrombosis in Pediatric Liver Transplantation, a 15-year retrospective study.
Chu K, Karnwal A, Cardona H, Hung A
Children's Hospital Los Angeles, Los Angeles, California, United states of america
Introduction: Vascular complications are common following pediatric liver transplantation (PLT) with an incidence of 7-10% for portal vein thrombosis (PVT) and 4-25% for hepatic artery thrombosis (HAT). 1 We aimed to analyze the incidence and factors associated with thrombotic complications after PLT at Children's Hospital Los Angeles.
Methods: After IRB approval, all patients who had PLT from 2000 to 2015 from were included in the study. We retrospectively collected demographic, perioperative and outcome data. Thrombosis was identified through chart review as well as imaging including ultrasound, doppler or CT scan up to 1 year after surgery. A univariate logistic regression was done for individual variables.
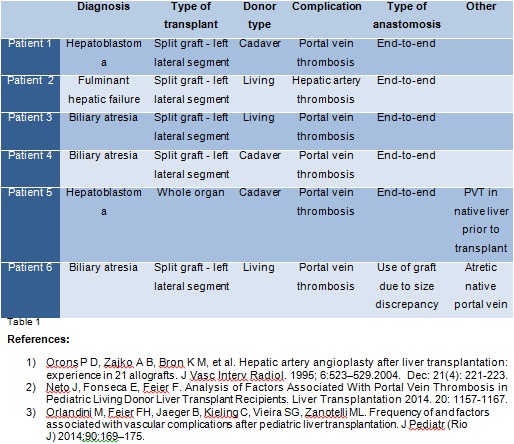
Results: A total of 156 PLTs were performed in the study period, of which, 14 were concurrent with kidney or small bowel transplant and 142 were solely PLTs. The average ICU length of stay was 170 hours (range 12-635) with 2 postoperative deaths. The commonest indication were cholestatic disorders n=76 (54%) followed by metabolic disorders n=21 (14.5%), Idiopathic n=21 (14.5%), Liver tumors n=17 (12%), Hepatitis n=5 (3.5%) and others 2 (1.5%). We found PVT in 5 patients 3.5% (5/142) and HAT 0.70% (1/142). Of the six patients with vascular complications, 50% (3/6) had a diagnosis of biliary atresia, 50% (3/6) had a living donor graft, and 33% (2/6) had a pre-existing vascular defect prior to transplant (Table 1). Interestingly, length of surgery, PELD scores, amount and type of blood products given and immediate post-operative coagulation status did not show any correlation with PVT or HAT. We utilized Firth penalized logistic regression to reduce bias due to small sample size.
Discussion: Although thrombotic events occur less frequently than bleeding complications after PLTs, they threaten patient and graft survival2. In addition, biliary atresia (BA), the leading indication for transplantation in children causes portal vein sclerosis, which results in technical difficulties during vascular reconstruction. In this study, 60% of PVTs (3/5) were associated with BA diagnosis. Of all thrombotic complications, 50% occurred in living donors and the other half in cadaveric donors. PVT and HAT are known to occur more commonly in children as compared to adults due to smaller caliber of vessels, split procedures, and involuntary development of high hematocrit. Other factors associated with PVT include size discrepancy between the donor and recipient vasculature, anastomotic kinks, low portal flow, and the presence of preoperative PVT 3. Our practice is to anticoagulate with Heparin and/or Dextran 40, when end-to-end anastomosis is performed under surgical guidance. While this could contribute to the lower incidence of PVT and HAT at our center, we also strive to maintain a post-operative hematocrit below 30 and INR between 1.5-2. In addition, consistency in surgical team and technique were other favorable factors at our center.
-
 GA1-48 Image 1
GA1-48 Image 1
Top










