
NM-243
Risk factor for post-induction hypotension in children presenting for surgery
1Wani T, 2Hakim M, 3Ramesh A, 4Rehman S, 5Majid Y, 6Miller R, 7Tumin D, 8Tobias J
1Nationwide childrens Hospital, King Fahd medical city, columbus, Ohio, Uinted states of america; 2Nationwide childrens Hospital, columbus, Ohio, United states of america; 3University of Nebraska medical centre, Omaha, NE, United states of america; 4University of west virginia, Morgantown, West virgi, United states of america; 5King fahd medical city, Riyadh, Eastern pr, Saudi arabia; 6Nationwide Childrens Hospital, Columbus, Ohio, OHIO; 7Natonwide Children's Hospital, columbus, Ohio, United states of america; 8Nationwide children's Hospital, Ohio State University College of Medicine, columbus, Ohio, United states of america
Background: Preoperative factors have been correlated with pre-incision hypotension (PIH) in children undergoing surgery, suggesting that PIH can be predicted through preoperative screening. We analyzed blood pressure (BP) changes 12 minutes after induction of anesthesia to assess the feasibility of predicting PIH in low-risk children without preoperative hypotension or co-morbid features.
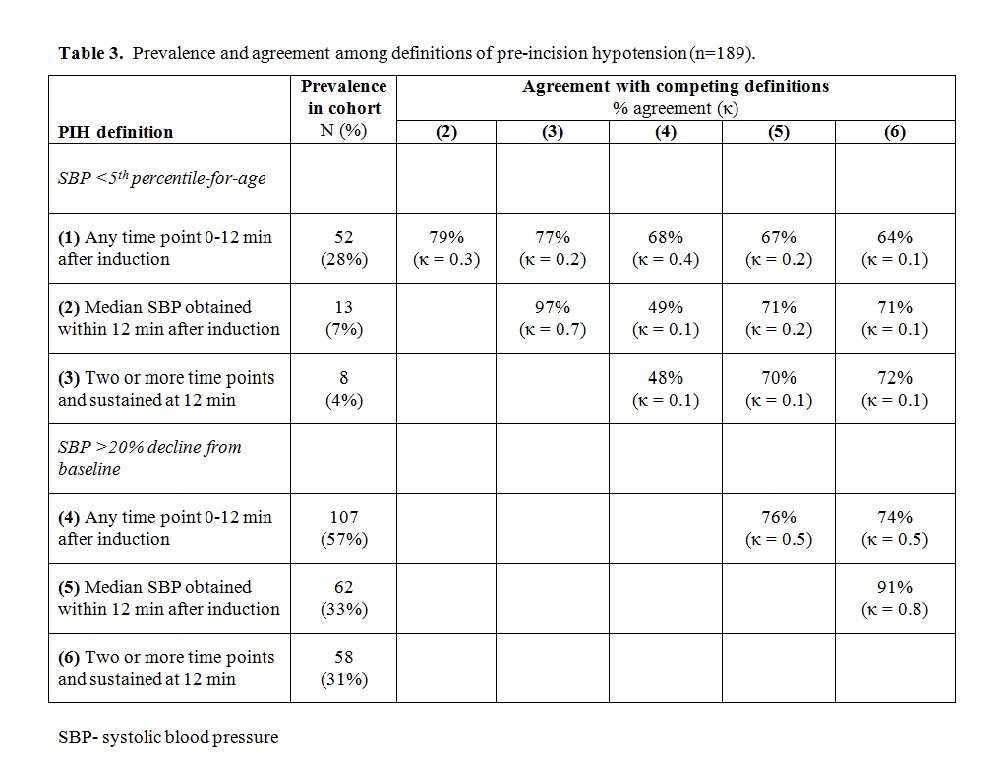
Methods: Patients age 2-8 years undergoing non-cardiac surgery were included in the study if they were ASA status 1-2, and had no preoperative hypotension (systolic blood pressure (SBP) <5th percentile for age). SBP was recorded at 3 minute intervals for 12 minutes after induction of anesthesia. We considered 6 definitions of pre-incision hypotension (PIH): (1) SBP <5th percentile for age at any time point, (2) at the median value, (3) at 2 or more time points including the final time point (sustained PIH); and a drop in SBP >20% from baseline (4) at any time point, (5) for the median value, or (6) at 2 or more time points including the final point. Pairwise agreement between definitions was assessed using the kappa statistic, where κ > 0.4 signified good agreement. Each outcome was predicted according to stepwise multivariable logistic regression including age, gender, type of induction, premedication use, preoperative SBP, preoperative heart rate, and body mass index.
Results: The analysis included 189 patients. PIH prevalence according to each definition ranged from 4% (definition [3]) to 57% (definition [4]). Pairwise agreement among the 6 definitions ranged from 49% to 91% agreement (Table1). Agreement was especially poor between measures based on SBP percentile-for-age and SBP percent decline from baseline. No sequelae of PIH were noted. On multivariable analysis, no covariates were consistently associated with PIH risk across all 6 definitions of PIH.
Conclusion: In a cohort of relatively healthy children, accurate prediction of PIH appears to be hampered by lack of agreement between definitions of PIH. Overall, PIH incidence was low when using accepted hypotension definition of SBP <5th percentile for age.
References:
1. Nafiu OO, Kheterpal S, Morris M, Reynolds PI, Malviya S, Tremper KK. Incidence and risk factors for preincision hypotension in a noncardiac pediatric surgical population. Paediatr Anaesth 2009;19:232-239.
2. Nafiu OO, Maclean S, Blum J, Kheterpal S, Cowan A, Tremper KK. High BMI in children as a risk factor for intraoperative hypotension. Eur J Anaesthesiol 2010;27:1065-1068.
3. Stewart M, Scattoloni J, Tazhibi G, Nafiu OO. Association of elevated preoperative blood pressure with preincision hypotension in pediatric surgical patients. Paediatr Anaesth 2016;26:844-851.
-
 NM-243 Image 1
NM-243 Image 1
Top










