
CR2-187
3D Models for Complex Congenital Heart Disease - A Game Changer?
1Lee J, 2Chhabada S
1Cleveland Clinic, Beachwood, Ohio, United states of america; 2Cleveland Clinic Foundation, Cleveland, Ohio, USA
Introduction
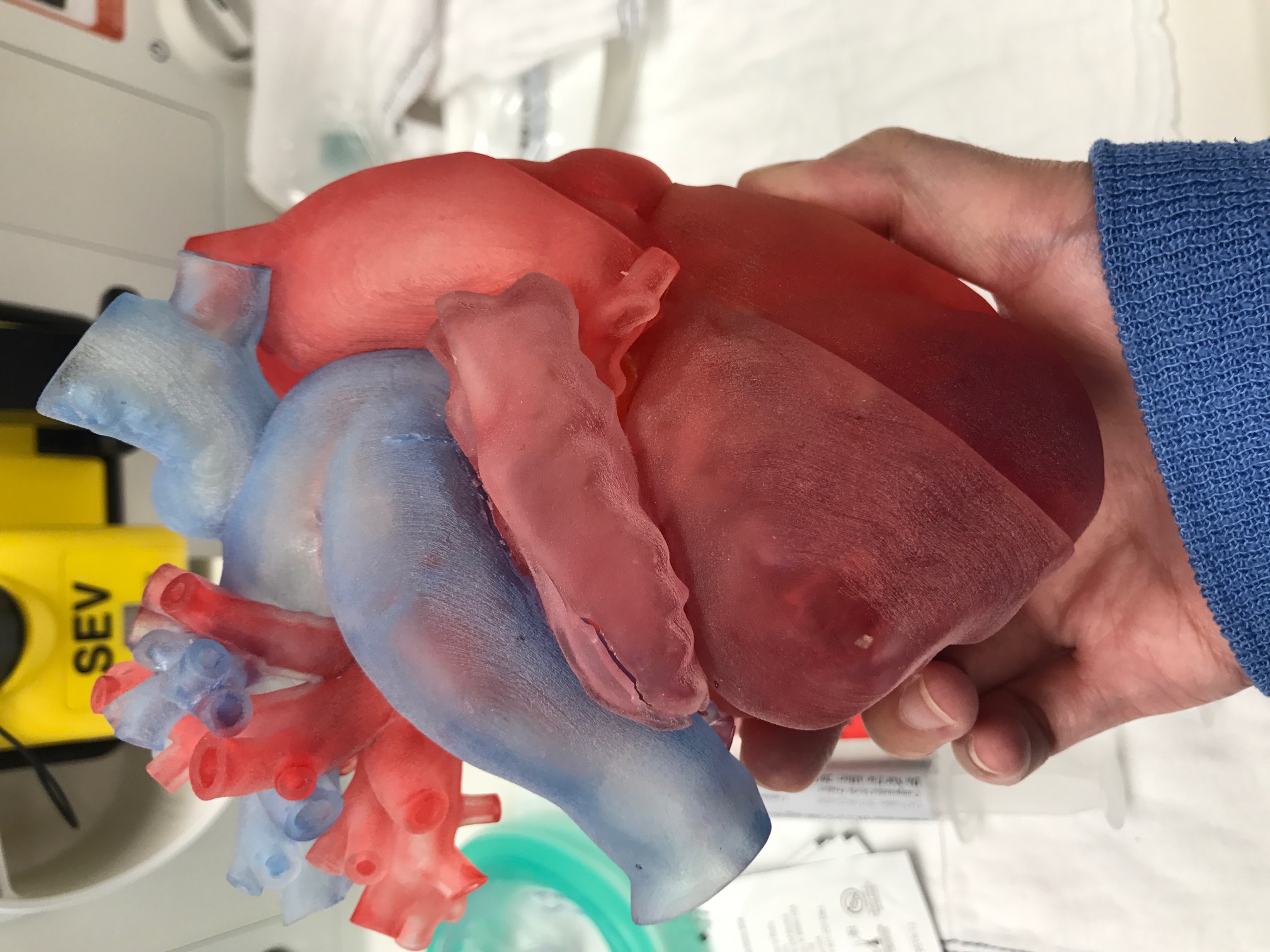
The technology of three-dimensional (3D) printing has recently been incorporated into the evaluation and surgical treatment of complex congenital heart disease (CHD). The growing sentiment among cardiac surgeons is that a 3D model helps increase confidence when making a surgical plan. We present a case where a life size 3D model of the patient’s heart played an integral role in his treatment.
Case Summary
The patient is a 10 year old male with a history of congenitally corrected TGA, double outlet right ventricle, pulmonary stenosis, VSD and complete AV block. His surgical history includes palliative repair with bidirectional Glenn, extracardiac nonfenestrated Fontan and placement of a pacemaker. He was initially evaluated for heart transplant due to failing Fontan physiology with protein losing enteropathy. A 3D model of his heart created from an MRI was presented at multidisciplinary conference, where it was determined that a one and a half ventricle repair would be feasible. Successful repair included takedown of the Fontan, intraventricular baffle of Gore-Tex connecting the left ventricle to the aorta through the VSD, Hemi-Mustard operation diverting the IVC to the tricuspid valve, augmentation of the left atrium with bovine pericardial patch, Glenn anastomosis left intact and creation of a valved right ventricle to pulmonary artery conduit.
Discussion
The management of complex CHD is challenging due to highly variable anatomy with a variety of surgical options. When discussing complex cases, using the 3D model can be instrumental for effective communication amongst a multidisciplinary team in order to formulate the best treatment plan. Visualizing the anatomy helps minimize the risk of unexpected intraop findings and avoid prolonged cardiac bypass and operative time. By enhancing understanding and communication, the 3D model also boosts the team’s confidence for surgery, which would have otherwise not been considered a feasible option.
Given the complexity and rarity of this case, the 3D model proved vital in discussions and forming a surgical plan. While there are limitations and challenges to the technology, it is an exciting tool that has great potential for understanding unique anatomy, communicating with colleagues, teaching trainees and fellows, and educating patients and families.
References:
Valverde I et al. Three-dimensional printed models for surgical planning of complex congenital heart defects: an international multicentre study. Eur J Cardio-Thoracic Surg 2017, 0: 1-10
Garekar S et al. Clinical application & multidisciplinary assessment of three dimensional printing in double outlet right ventricle with remote ventricular septal defect. World J for Pediatric and Congenital Heart Surg 2016, 7(3): 344-350
Valverde I. Three-dimensional printed cardiac models: applications in the field of medical education, cardiovascular surgery, & structural heart interventions. Rev Esp Cardiol 2017, 70(4): 282-291
-
 CR2-187 Image 1
CR2-187 Image 1
Top










