
AIR-15
Not everything that wheezes is asthma: An unusual presentation of a juvenile xanthogranuloma.
Acosta S, Waller E
UNC Hospital, Chapel Hill, NC, USA
Introduction:
Juvenile xanthogranulomas (JXGs) are rare benign tumors that typically present at birth but can affect all ages. JXGs are most commonly cutaneous lesions, and rarely present extracutaneous. We present an unusual case of a JXG lesion in the trachea, causing significant respiratory symptoms and requiring surgical resection.
Case:
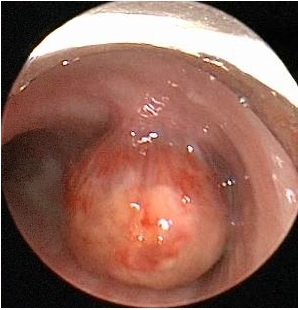
A 4 y/o female recently diagnosed with asthma 4 months prior presented to an OSH with respiratory distress. This was her second hospitalization for presumed asthma exacerbation in <3 weeks. She rapidly deteriorated despite maximal medical therapy and was intubated with a 4.5 cuffed ETT. Flexible bronchoscopy demonstrated a tracheal mass pedicled at the anterior wall and obscuring the right mainstem bronchus (RMB). The pt was transferred to UNC for surgical management.
A multidisciplinary team including pulmonary, ENT, anesthesia, and cardiac surgery was assembled. Due to the pt’s size and the location of the tumor, it could not be resected with the ETT in place. A propofol-based anesthetic was used, and spontaneous respirations maintained. Cardiac surgery and ECMO teams were on standby. The ETT was removed, and ENT placed a 3.7 rigid bronchoscope into the trachea under direct laryngoscopy.
The tumor was excised piecemeal using a CO2 laser fiber. The pt experienced frequent desaturations requiring BMV, secondary to intermittent ball-valve effect of the tumor on the RMB, obliterating ventilation to the right lung and causing significant V/Q mismatch. The tumor was successfully removed, and the pt was extubated. She was weaned to RA by POD2 and discharged home on POD3. Subsequent pathology report demonstrated JXG. At 6-week follow-up, the pt’s mother reported resolution of her asthma symptoms.
Discussion:
While there are common causes of wheezing in children such as reactive airway disease, rare and serious etiologies must be considered. Less common causes include congenital abnormalities, foreign body aspiration, cystic fibrosis and tumors.
Children with recurrent or unexplained wheezing unresponsive to bronchodilators should undergo further testing, such as CXR. However, if foreign body aspiration is suspected, rigid bronchoscopy should be performed due to the low sensitivity for diagnosis with CXR.
Anesthetic considerations for rigid bronchoscopy include available personnel, anesthetic induction technique and ventilatory strategy. Induction of anesthesia utilizing inhalational anesthetics or IV medications are dependent on provider comfort. Maintenance of spontaneous ventilation is critical. A plan should be in place in case of loss of the airway, and ECMO or CPB may need to be considered.
References:
1. Pajaziti et al. BMC Research Notes 2014, 7:174
2. J Pediatr Hematol Oncol Volume 36, Number 8, November 2014
3. Am Fam Phys. 2008 Apr 15;77(8):1109-1114.
4. Pediatric Anesthesia. 2004 14: 84–89
-
 AIR-15 Image 1
AIR-15 Image 1
Top










