
CA-33
Dexmedetomidine Pharmacokinetics and a New Dosing Paradigm in Young Children Supported With Cardiopulmonary Bypass
1Zimmerman K, 2Wu H, 3Laughon M, 1Greenberg R, 4Walczack R, 5Schulman S, 1Smith B, 1Hornik C, 1Cohen-Wolkowiez M, 1Watt K
1Duke University; Duke Clinical Research Institute, Durham, NC, USA; 2Duke Clinical Research Institute, Durham, NC, USA; 3University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 4Duke University, Durham, NC, USA; 5University of California, San Francisco, San Francisco, CA, USA
Introduction: Dexmedetomidine is increasingly used in infants and children with cardiac disease, during cardiopulmonary bypass (CPB) and in the postoperative period. Despite its frequent use, optimal dosing of dexmedetomidine in the setting of CPB has not been identified, but is expected to differ from dosing in those not supported with CPB.
Study aim: We aimed to characterize the effect of CPB on dexmedetomidine pharmacokinetics (PK) in young children and to identify optimal dosing in this setting.
Methods: Following IRB approval, we performed an open-label, single-center PK and safety study of dexmedetomidine in participants ≤ 36 months age who were administered dexmedetomidine per standard of care, initiated at 0.5ug/kg/h without a loading dose in the pre-CPB period. We analyzed dexmedetomidine PK data using nonlinear mixed effects modeling with NONMEM software. We compared model-estimated PK parameters to historical controls and investigated CPB-related factors that influenced PK estimates. We used the final model to simulate dosing recommendations that targeted a concentration of 0.6 ng/mL based on prior safety and efficacy data. The incidences of hypotension and bradycardia in the post-CPB period were evaluated.
Results: We collected 213 dexmedetomidine plasma samples from 18 participants. Twenty-eight samples (13%), mostly collected during the pre-CPB and early CPB periods, were below the lower limit of quantification (BQL). Participants had a median (range) age of 3.3 months (0.1, 34.0) and underwent CPB for 161 minutes (63, 394).
.
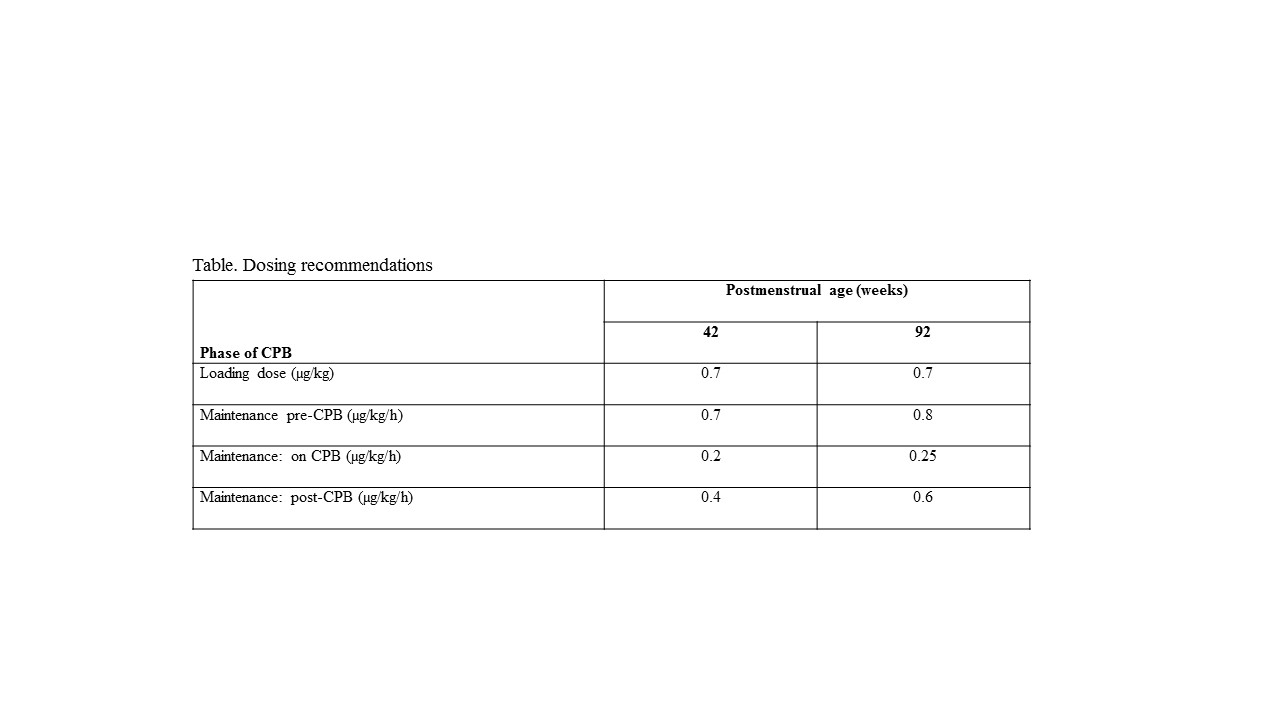
We estimated a clearance (CL) of 13.4 L/h/70 kg during CPB, compared to 42.1 L/h/70 kg in historical infants and young children not supported with CPB. No specific CPB-related factor had a statistically significant effect on PK. Dosing simulations designed to attain the target concentration by the time of CPB initiation suggested the need for a loading dose in the pre-CPB period followed by maintenance infusions based on post-menstrual age (Table). . We identified no association between dexmedetomidine exposure and selected adverse events (P=.13).
Discussion: The high proportion of BQL samples early in the study period and prolonged time period required to attain target concentrations underscore the need for an appropriate loading dose of dexmedetomidine to achieve a therapeutic concentration before initiation of CPB. CPB is associated with lower dexmedetomidine CL in infants and young children compared to those who do not undergo CPB. Further study should more closely investigate specific CPB-related factors that may influence CL during CPB.
Conclusion: While a loading dose is often necessary to attain target concentrations prior to initiation of CPB in young children, dosing of dexmedetomidine during CPB should account for decreased drug clearance in this setting.
-
 CA-33 Image 1
CA-33 Image 1
Top










