
RRA-7
STBUR: Sleep Trouble Breathing and Unrefreshed questionnaire: Evaluation of screening tool for post-anesthesia care and disposition.
1Yaport M, 2Simpao A, 2Tan J, 2Wasey J, 2Lingappan A, 2Ahumada L, 2Song B, 2Wu L, 2Rehman M, 2Dubow S, 2Galvez J
1University of Pennsylvania, Philadelphia, PA, USA; 2The Children's Hospital of Philadelphia, Philadelphia, PA, USA
INTRODUCTION: The Snoring, Trouble Breathing and Un-Refreshed (STBUR) Questionnaire is a 5-question screening tool for pediatric sleep-disordered breathing and risk for perioperative respiratory adverse events (PRAE) in children.(1, 2) We incorporated STBUR screening in the pre-anesthesia evaluation of outpatients scheduled for surgical procedures at The Children’s Hospital of Philadelphia (CHOP). We evaluated STBUR’s performance in risk-stratification for post-anesthesia events that can impact scheduling patients in ambulatory surgical settings.
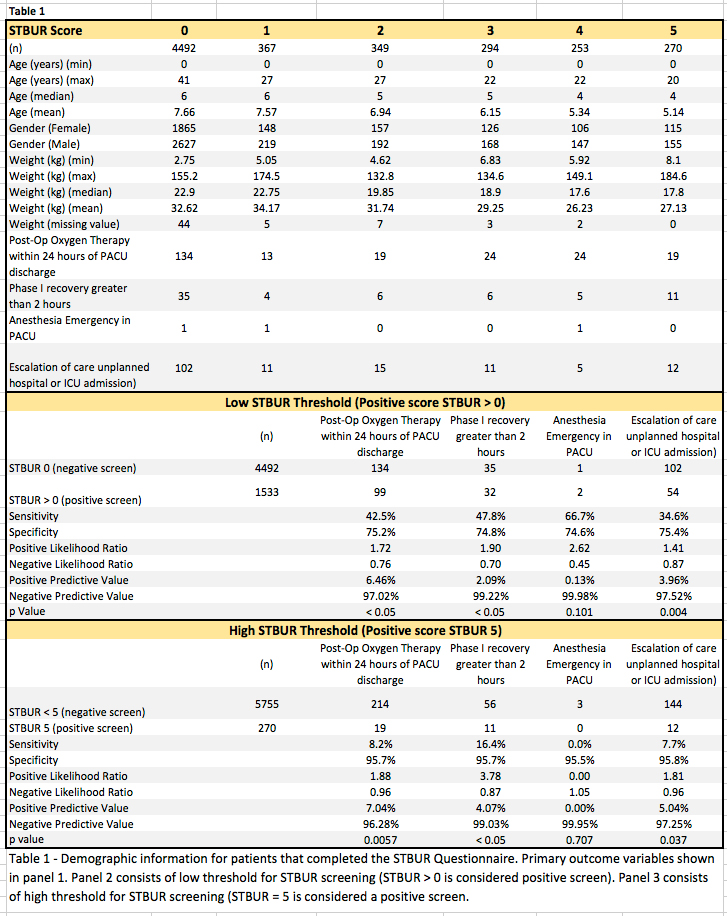
METHODS: This quality improvement (QI) study of all children who completed a pre-anesthesia evaluation before elective surgery at CHOP did not require IRB oversight. We retrieved perioperative data from the clinical data warehouse. Positive STBUR was defined in two categories: low threshold positive STBUR>0 and negative STBUR=0, high threshold positive as STBUR=5 and negative as STBUR<5. The primary outcomes were 1. Oxygen requirement after PACU discharge, 2. Phase 1 recovery greater than 2 hours, 3. Anesthesia emergency in PACU and 4. Unplanned hospital or ICU admission. Statistical analysis was conducted with R Statistical software. Univariate analysis was performed. Sensitivity, specificity, and predictive values were calculated. A p value of < 0.05 was considered statistically significant.
RESULTS: 6,025 patients completed pre-operative STBUR questionnaire in the pre-operative evaluation. 1,533 patients had a positive STBUR (Table 1), of which 99(42%) required oxygen following PACU stay until hospital discharge, 32(48%) spent more than 2 hours in phase 1 recovery, 2(67%) had anesthesia emergency activation in PACU and 54(35%) had an unplanned hospital or ICU admissions compared to patients with STBUR 0. We observed a statistically significant increase in the post-operative oxygen therapy, phase 1 recovery greater than 2 hours and unplanned hospital admission for patients with positive STBUR screening (Score>0 ) as compared to negative STBUR screening (Score=0). The sensitivity of the screening tool ranges from 8% to 48% depending on the criteria set for a positive screen (i.e. STBUR>0 or STBUR=5)(Table 1).
CONCLUSION: The STBUR tool correlated with the higher prevalence of three of the outcome variables. The STUBUR questionnaire identifies patients at higher risk for prolonged phase 1 recovery, oxygen therapy requirement and escalation of care (Table 1). However, the clinical significance may be limited due to its low sensitivity and positive predictive value. A STBUR score of 0 may be useful, as it does have a high negative predictive value and specificity. STBUR may be useful as a screening tool to optimize scheduling of high-risk patients in a way that minimizes the impact of a prolonged stay in PACU. We believe that the predictive value can improve by with additional predictor variables.
REFERENCES:
1. Tait et al. Paediatr Anaesth. 2013.
2. Tait et al. Paediatr Anaesth. 2016.
-
 RRA-7 Image 1
RRA-7 Image 1
Top










