
GA3-69
The clinical implications of pulse oximeter sensor accuracy in the sleep laboratory
Twite M, Ing R, Boucharel W
University of Colorado, Aurora, CO, USA
Introduction
Pulse oximetry is a core monitoring modality in medicine. Aoyagi first described its use in 1974(1) and since then it has become widely accepted as a standard of care monitor in hospital medicine. However, recent clinical observations of large differences in pulse oximetry readings on the same patient with different sensors has raised questions of accuracy.(2)
Background
Children with sleep-disordered breathing often undergo a sleep study to help establish a diagnosis and determine therapeutic options which may include; supplemental oxygen therapy, non-invasive respiratory support, and tonsillectomy. A sleep study involves multi-modality monitoring including pulse oximetry. The sleep laboratory at our hospital uses two different pulse oximeter sensors to measure peripheral oxygen saturations (SpO2). Often, these sensors will provide different readings that make it very difficult to interpret the sleep study data.
One source of inaccuracy may be related to the pulse oximeter sensor itself. Pulse oximeter sensors use two light emitting diodes (LEDs) of specific and differing wavelength (660 and 940 nm) to measure the combined absorption of oxyhemoglobin and deoxyhemoglobin. The ratio of absorption at these two wavelengths is called the R-value, and is compared with R-values stored in the pulse oximeter monitor. Should the wavelength of the light emitted by one or both LEDs alter, the degree of absorption will alter and the R-value will change. At lower saturations, the SpO2 error will be greater as the absorption of reduced hemoglobin is much more sensitive to wavelength errors. The Lightman® (The Electrode Co. Ltd, Monmouthshire, UK) is a portable microspectrophotmeter that uses an internal diode-array to measure the exact emission spectra of the LEDs in pulse oximeter sensors. (3)
Hypothesis
The pulse oximeter sensors being used for sleep studies have varying accuracy due to the quality of the LEDs.
Method
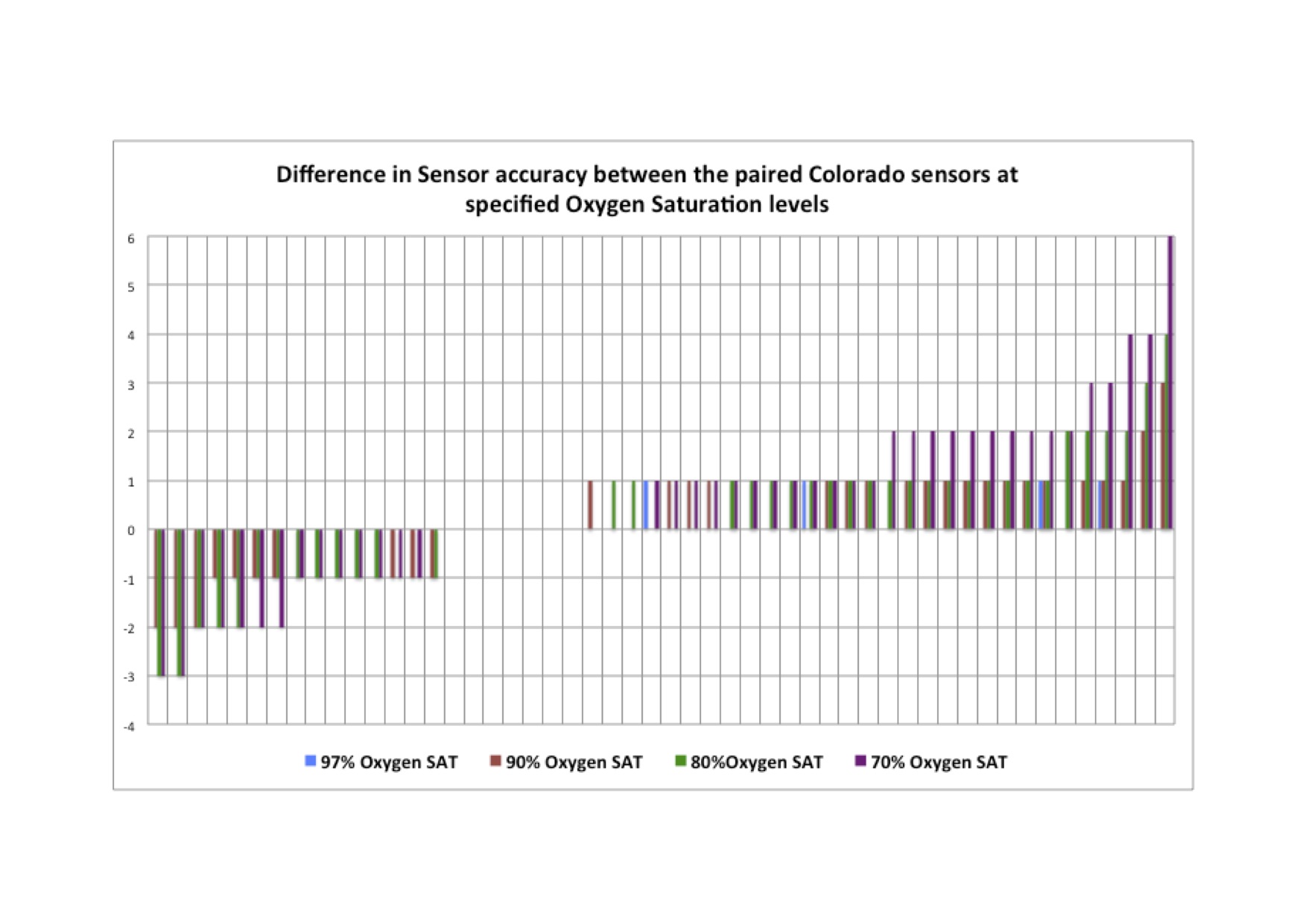
This IRB approved, prospective study collected 50 paired sensors (Nelcor and Masimo) after they had been used for a sleep study. The sensors were then analyzed using The Lightman®, to determine their accuracy and the bias of every sensor at differing SpO2 values.
Results
Figure 1 shows the considerable range in the accuracy of the sensors analyzed.
Conclusion
The data presented here shows that pulse oximetry may not always be an accurate measure of SpO2 and this could lead to inappropriate therapeutic decisions being made. Further study is needed to understand the extent of this issue.
Refs
1. Severinghaus JW. Aoyagi T: Discovery of pulse oximetry. Anesth Analg. 2007;105
2. Ross PA et al. Accuracy of pulse oximetry in children. Pediatrics. 2014;133:22-9.
3. Milner QJ, Mathews GR. An assessment of the accuracy of pulse oximeters. Anaesthesia. 2012;67:396-401.
-
 GA3-69 Image 1
GA3-69 Image 1
Top










