
OS2-145
Noninvasive Ventilatory Monitoring in Children with Obstructive Sleep Apnea Following Adenotonsillectomy
1Monitto C, 1Kerns N, 1Hsu A, 1Duval-Arnould J, 1Zsido L, 2Yaster M, 1Gottschalk A
1Johns Hopkins Medical Institutions, Baltimore, MD, USA; 2University of Colorado-Anschutz Medical Campus, Children’s Hospital Colorado, Aurora, CO, USA
INTRODUCTION: Post-operative respiratory depression is a catastrophic and potentially preventable consequence of analgesia, anesthesia, and surgery, particularly in children diagnosed with sleep disordered breathing. In pediatrics, the most commonly used monitors, pulse oximetry (SaO2), impedance pneuomography (RR), and capnography (ETCO2 and RR) are often unreliable and may miss airway obstruction and/or hypoventilation. We hypothesized that 2 new devices, the ExSpironâ„¢ monitor, a device capable of monitoring tidal volume (TV), RR, and minute ventilation (MV) and the SenTecâ„¢ digital monitor, a transcutaneous CO2 (TC-CO2) monitor, would be capable of detecting episodes of respiratory insufficiency not identified by current monitoring techniques.
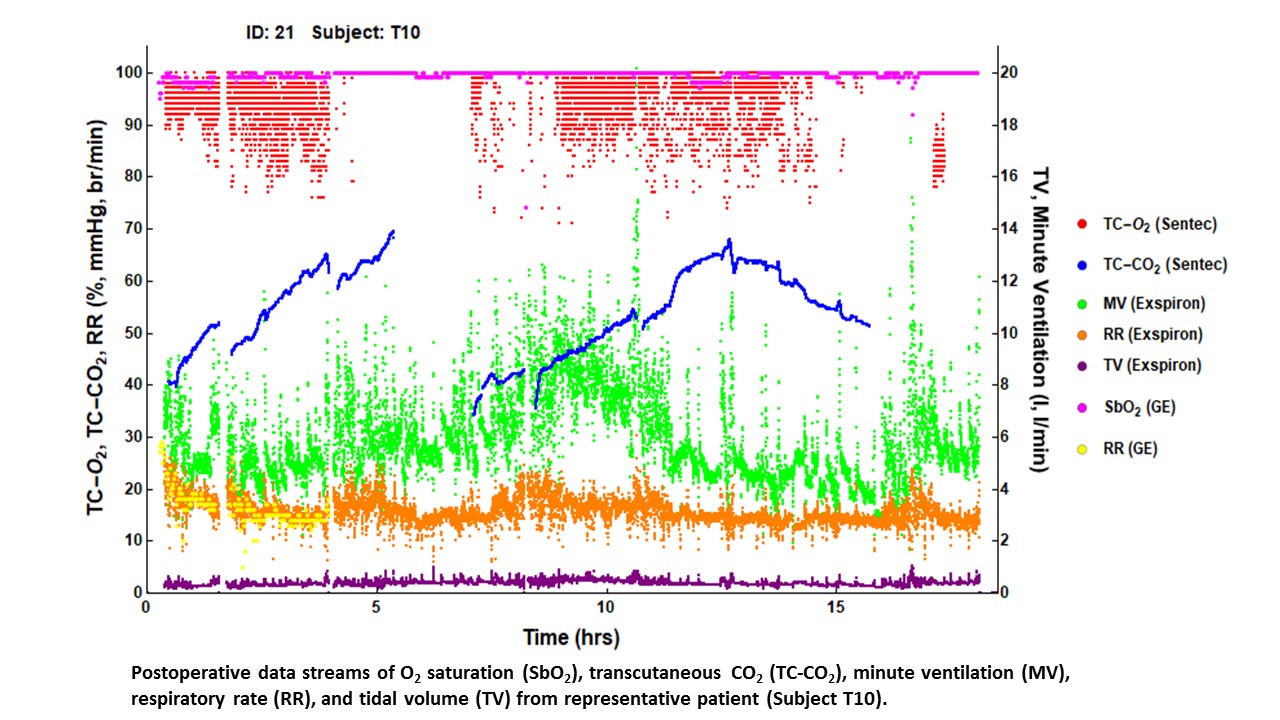
METHODS: Following IRB approval, informed consent and when appropriate patient assent, children (3-21 years of age) undergoing adenotonsillectomy (T&A) for moderate-to-severe obstructive sleep apnea admitted for overnight observation were enrolled. Upon completion of surgery, while still intubated, the ExSpiron™ monitor was secured on the patient’s chest and calibrated to the anesthesia machine MV. Upon arrival to the PACU the SenTec™ Digital Monitor was also placed and calibrated. Data from both monitors was collected during the first postoperative night. Continuous pulse oximetry and pain and sedation medication usage data were also collected from the hospital-wide GE monitoring system and EPIC. Data from these multiple streams were generated using sampling rates of 1 second to 1 minute, and were overlaid using the common timestamp.
RESULTS: Data streams of up to 20 hrs duration from 11 subjects (6 male/5 female, average age 6.1+2.4 y, 31.5+19.6 kg, preoperative respiratory distress index: 3-28 events/hour) were initially examined. While TC-CO2 data was not perfectly continuous across the entire monitoring period, it was the least variable over time of all the physiologic parameters obtained. For 3 of 11 T&A patients, TC-CO2 exceeded 60 mmHg for sustained periods (>30 min) without associated hypopnea or hypoxia revealed by contemporaneous monitoring.
CONCLUSIONS: While TC-CO2 monitoring was limited in its ability to provide a reliable continuous monitor, it is clearly a valuable research tool with regard to demonstrating the level of safety of the perioperative respiratory state. In our preliminary sample, it detected episodes of respiratory insufficiency not identified by standard monitoring and revealed that almost 30% of subjects studied experienced periods of respiratory compromise not detected by respiratory rate or pulse oximetry monitoring in the early postoperative period.
-
 OS2-145 Image 1
OS2-145 Image 1
Top










