
NM-253
Air in Patient IV Lines – Fluid Warmers, Syringes and Other Clinical Interventions that Increase Air Burden for Patients
Tirotta C
Nicklaus Children's Hospital, Miami, FL, USA
Abstract: Air in Patient IV Lines – Fluid Warmers, Syringes and Other Clinical Interventions that Increase Air Burden for Patients
Objective
Air in intravenous (IV) lines can be harmful, even in small amounts. The risk is greatly magnified in pediatric patients with congenital heart disease. This patient population is at particular risk during surgery, when standard IV line air filters are not feasible for the administration of blood products or medications. Understanding the triggers to air entry, clinicians can alleviate the air burden and stop preventable air from reaching their patients. Several devices are now on the market that purport to effectively remove air from IV lines. One is the ClearLine IV from ClearLine MD (Woburn, MA). The ClearLine IV consists of the control unit and the disposable cartridge. Air is detected in the IV line by a software-controlled ultrasound sensing technology. When air is detected, the flow is diverted to a collection chamber. When air is no longer detected, flow to the patient is resumed. The device purports to remove air bubbles as small as 25 microliters at flow rates of up to 400 ml/minute. The primary objective is to identify the triggers of air entrainment due to IV manipulations and understand its delivery in a typical clinical setting.
Method
A multicenter, prospective observational study was conducted at four different academic institutions. After informed consent was obtained, the ClearLine IV was inserted into the IV line of adult and pediatric surgical patients undergoing the procedures. Practitioners conducted the anesthetic in their normal fashion. IV fluid was administered at a constant flow rate or via boluses given over 30-60 seconds. The start of the IV and the commencement of the ClearLine IV was noted. Blood warmers were used at the discretion of the practitioners. Fluid administration was recorded by noting volume and duration of administration. At the end of the case, data was collected from the device on the frequency, duration and amount of air captured along with clinical manipulations of the IV line.
Results
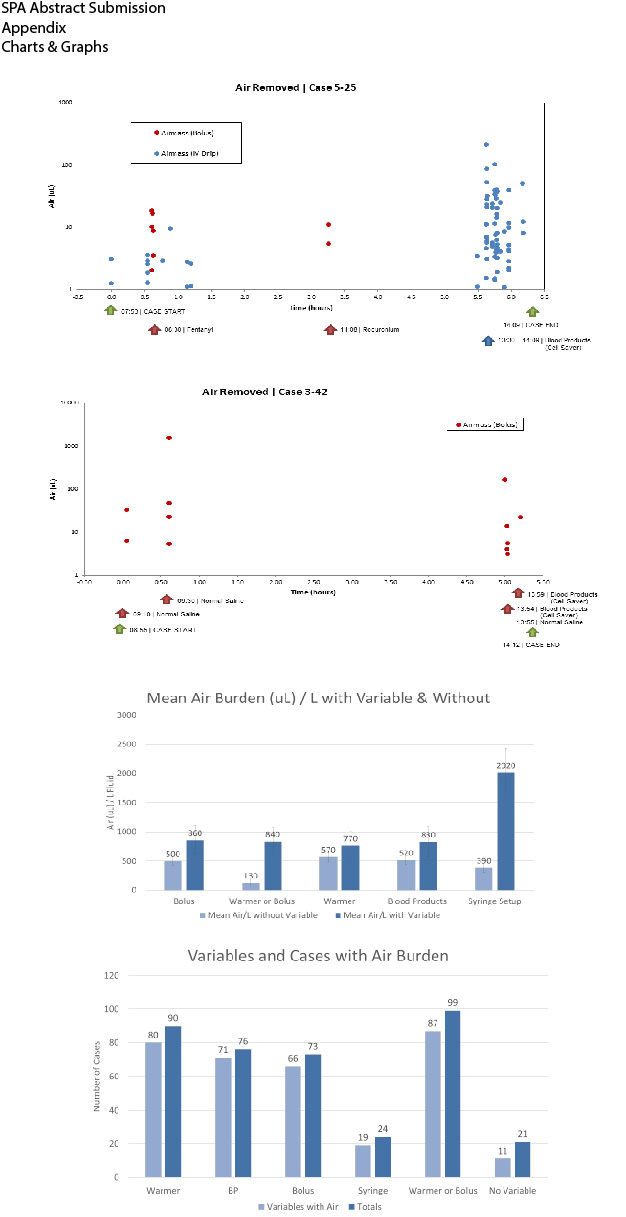
Data from 120 patients was included in this analysis. Air burden was detected in 52% of the cases. Use of a fluid warmer or bolus increased the likelihood of air burden to 79%. For every 10mL of blood products administered, the risk increases by 0.5%. The high air model (1ml air/1L fluid) concludes the baseline probability of high air to be 0%. Use of a warmer or a bolus resulted in high air burden in 50% of the cases. The inclusion of a syringe setup increased the probability of air introduced into the IV line to be 20%.
-
 NM-253 Image 1
NM-253 Image 1
Top










