
OS2-141
Incidence and Risk Factors Associated with Acute Kidney Injury in the Pediatric Surgical Population
Wingert T, Ren W, Grogan T, Hofer I
UCLA, Los Angeles, CA, USA
INTRODUCTION: Pediatric acute kidney injury (AKI) is increasingly being recognized as a source of major morbidity and mortality. Studies of incidence and risk factors for AKI are limited to children undergoing cardiac surgery and those admitted to intensive care units1,2. Our study aim was to evaluate the incidence of AKI and risk factors in the non-cardiac pediatric surgical population.
METHODS: All patients 18 years and under who underwent non-cardiac surgery or procedures, between March 2013 and September 2017 at UCLA Medical Center and its affiliated surgery centers were identified. Cases were included if there was no history of end-stage renal disease (ESRD), a baseline serum creatinine (SCr) level within 6 months before surgery existed and SCr value was measured within 14 days after surgery. The Kidney Disease: Improving Global Outcomes (KDIGO) criteria were used to define AKI. Laboratory and descriptive data were gathered from the electronic medical record regarding potential risk factors including: age, ASA status, history of prematurity, congenital heart disease (CHD), and chronic kidney disease (CKD). Univariate and multivariate analyses were performed examining AKI both as a binary and ordinal outcome. Significance of associations were evaluated using Spearman rank correlation.
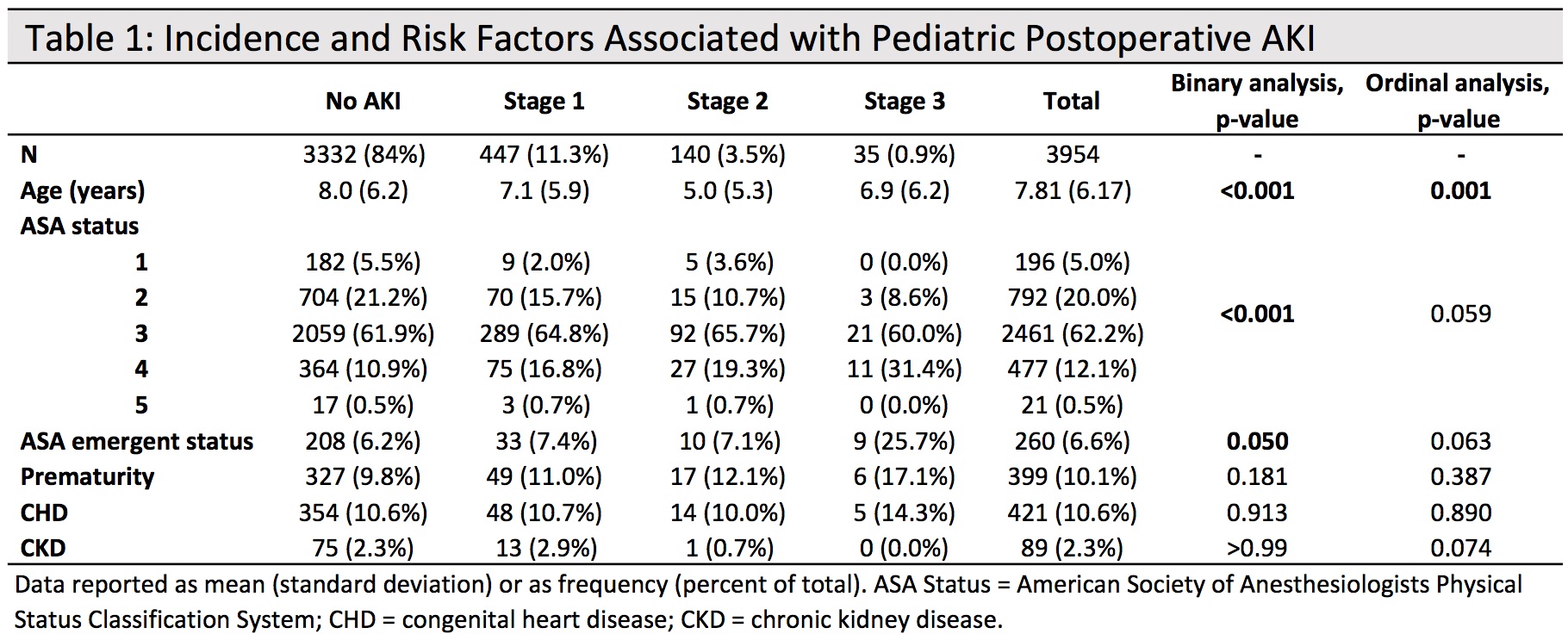
RESULTS: A total of 24,185 non-cardiac surgeries or procedures were performed during the 4.5-year period. After excluding for the above criteria, 3954 cases were analyzed. An overall 15.7% incidence of postoperative AKI was observed, with incidence of 11.3%, 3.5%, and 0.9% respectively of KDIGO stages 1, 2, and 3. Univariate analyses are seen in Table 1. Multivariate regression demonstrated each year decrease in age was associated with a 3% increased risk of AKI, after adjusting for ASA, prematurity, CHD, and CKD (p<0.001). Subgroup analysis of children who developed postoperative AKI revealed that younger patients were 5% more likely to have more severe AKI by an increased risk of 5% with each year decrease in age (p=0.002).
DISCUSSION: Based on data from a single institution, AKI is a morbidity that occurs frequently in the pediatric surgical population. Additionally, based on studies of AKI in pediatric subpopulations and adults there is reason to believe that AKI is associated with longterm morbidity and mortality1,3. Further research is needed to better understand causative factors and associations with other outcomes.
CONCLUSION: In an academic center population, pediatric AKI after non-cardiac surgery appears to occur with increased frequency and severity with younger age.
REFERENCES:
1. Kaddourah et al. Epidemiology of AKI in Critically Ill Children and Young Adults. NEJM 2017;376:11-20.
2. AlAbbas et al. Epidemiology of cardiac surgery-associated AKI in neonates: a retrospective study. Pediatr Nephrol 2013;28:1127–1134.
3. Blinder et al. Congenital heart surgery in infants: effects of AKI on outcomes. J Thor CV Surg. 2012;143:368–74.
-
 OS2-141 Image 1
OS2-141 Image 1
Top










