
NM-230
Nasotracheal Tube Damage During Craniofacial Surgery: an airway oddity
1Huynh P, 2Bell M, 2Flotildes K
1Harbor-UCLA Medical Center, Torrance, California, USA; 2Children's Hospital Los Angeles, Los Angeles, California, USA
Nasotracheal tube placement provides a patent airway and protects from aspiration of blood during oral and craniofacial surgery. Due to the proximity of surgical saws and instrumentation, damage to the endotracheal tube can range from cuff rupture to total transection. Intraoperative replacement of the endotracheal tube under these circumstances can be challenging. We report a case of nasotracheal tube rupture during a surgically assisted rapid palate expansion (SARPE) resulting in a large airway leak and culminating in replacement of the endotracheal tube in the surgical field.
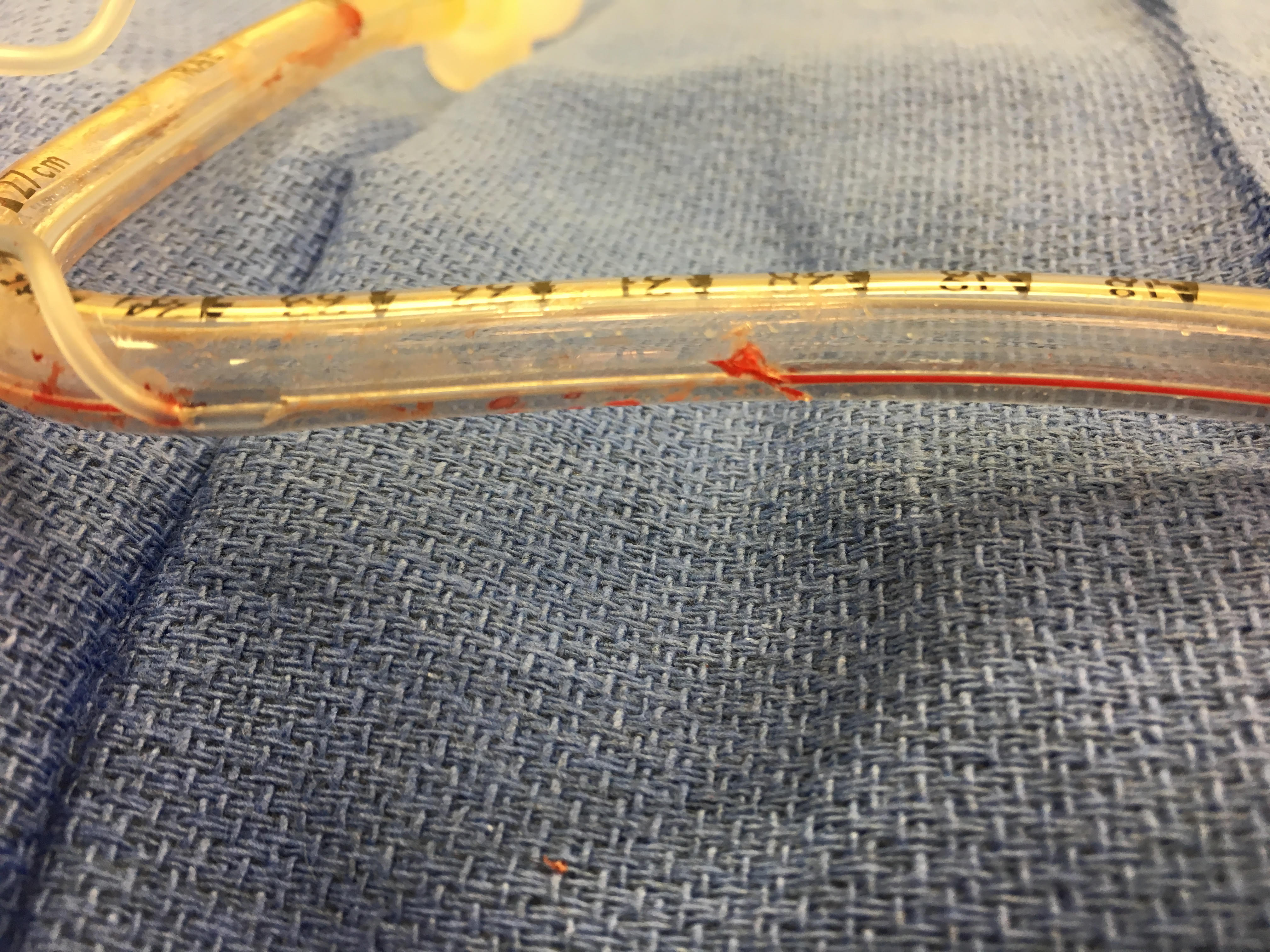
Presented is a 14 year old male with previous repair of bilateral cleft lip and palate who presented for SARPE. After receiving midazolam, general anesthesia was induced with lidocaine, fentanyl, propofol, and rocuronium. Nasotracheal intubation was performed with a 6.0 cuffed RAE tube. Surgery commenced. One hour later, a sudden large leak was detected. After verifying that the anesthesia circuit was intact, the pilot balloon was checked and held air. An intact pilot balloon was suggestive of an intact cuff. Direct laryngoscopy, followed by fiberoptic bronchoscopy (FOB), confirmed appropriate position of the ETT but revealed a defect in the wall. The nasal ETT was replaced under direct laryngoscopy. Later examination demonstrated a defect along the channel between the pilot balloon and the cuff. The channel had filled with blood and clotted. Thus, the pilot balloon held air, but the cuff was deflated.
This case report highlights a low frequency, high acuity complication that can occur during craniofacial surgeries – nasotracheal tube damage. Early recognition and swift intervention are essential to patient safety. Etiologies such as a leak from the circuit or anesthesia machine must be quickly ruled out. Cuff integrity and tube placement must be confirmed. This can occur via direct laryngoscopy or FOB. Theoretically, cuff damage can be identified by inflating the pilot balloon. The unique teaching point of this case report is that an intact pilot balloon that holds air does not necessary mean that the cuff is intact and holding air. No prior incidence of this occurrence has been reported in the literature.
The next step is managing an airway with a damaged nasotracheal tube. High gas flows and throat packing can be temporizing, but do not prevent aspiration. Endotracheal tube replacement is ideal, but
not easy in a bloody surgical field. Airway adjuncts can facilitate tube replacement. Lastly, one must be prepared for a surgical airway in the event of failure to oxygenate and ventilate.
1) Balakrishnan M, et al. Endotracheal tube damage during head and neck surgeries as a result of harmonic scalpel use. Anaesthesiology. 2005; 102:870-1.
2) Bang E, et al. Damage to Endotracheal Tube during Lefort I Osteotomy – A Case Report. Korean Journal of Anesthesiology. 2007;53(4):516-519.
-
 NM-230 Image 1
NM-230 Image 1
Top










