
NM-304
Congenital Heart Surgery in Patients with Sickle Cell Trait on Cardiopulmonary Bypass: Is Exchange Transfusion Indicated?
1Chacon-Portillo M, 1Mossad E, 2Beckerman Z, 1Zea-Vera R, 1Binsalamah Z, 1Adachi I, 1Mery C, 1Imamura M, 1Heinle J, 1Fraser Jr. C
1Texas Children's Hospital, Houston, Texas, United states; 2Emory University School of Medicine, Atlanta, Georgia, United states
Introduction: Current practices on sickle cell trait (SCT) patients are based mostly on adult homozygous sickle cell disease studies.
Aim: To evaluate whether exchange transfusion (ET) prevents complications in pediatric patients with SCT and congenital heart disease undergoing cardiopulmonary bypass (CPB) surgery.
Methods: Data from all patients with SCT diagnosis who underwent CPB surgery were collected from 1995 through 2016. Demographic information, CPB intraoperative measurements (i.e., regional cerebral oxygen saturation (RSO2), nasopharyngeal temperature °C, pH), and the number of blood product units given were collected. The on-pump hemoglobin S% was calculated based on the patient’s weight, preoperative hematocrit and hemoglobin S%, and estimated blood volume. Patients were separated into groups: a) non-ET and b) ET. Postoperative complications were collected and a composite outcome was created.
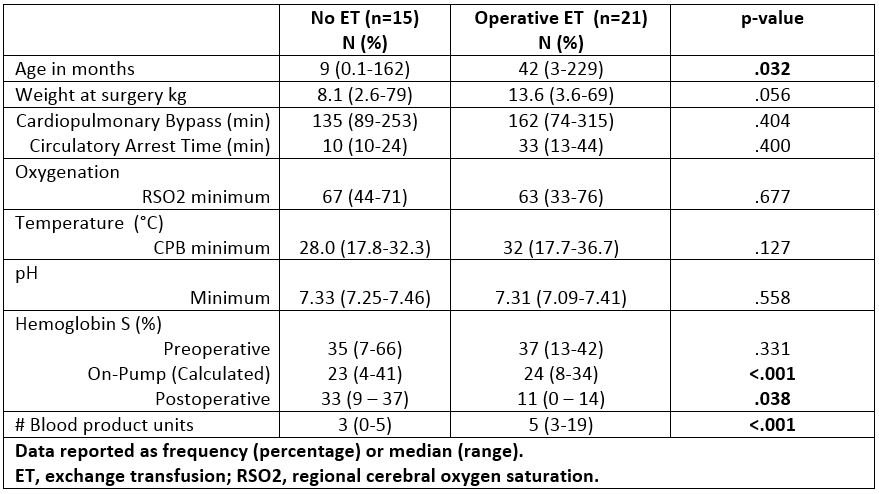
Results: A total of 36 patients (15 [42%] non-ET patients and 21 [58%] ET patients) were included, 27 (75%) had SCT and 9 (25%) had SCT and thalassemia. ET patients were older (42 [3-229] vs 8 [0.1-162] months, p=.032) than non-ET patients (Table 1). On-pump hemoglobin S% was higher in the ET group, 24% (8-34) vs 23% (4-41) in the non-ET group (p<.001). Postoperative hemoglobin S% was lower in the ET group, 11% (0-14) vs 33% (9-37) in the non-ET group (p=.038). Minimum CPB temperature, RSO2, and pH were comparable between groups. The ET group was given more blood products, 5 (3-19) vs 3 (0-5) the non-ET group (p<.001).
A total of 6 complications occurred in different patients: 2 acute chest syndromes, 1 vaso-occlusive event, 1 hemolytic anemia, 1 thrombocytopenia, and 1 hypoxic-ischemic brain injury. The incidence of the composite outcome was comparable between groups with 2 (13%) in the non-ET group and 4 (19%) in the ET group (p=.999). Patients with SCT complications had a longer CPB time (265 [122-299] vs 135 [74-315] minutes, p<.001), lower minimum RSO2 (59 [61-67] vs 66 [33-76], p<.001), lower minimum temperature (26.8°C [17.7-32.2] vs 29.4°C [17.8-36.7], p<.001), and minimum pH (7.29 [7.09-7.34] vs 7.34 [7.24-7.46], p<.001).
Discussion: In this retrospective single-center study, ET was not associated with a decrease in SCT associated complications in patients with congenital heart disease undergoing CPB procedures. Current practice is to perform ET to reduce hemoglobin S levels below 30% in patients undergoing high-risk procedures such as CPB surgery. Most studies describe sickle cell disease predominant populations, the largest sickle cell cohort includes only 4 SCT patients (Yousafzai et al., Circulation, Jan 5;121(1):14-9 2010). In our SCT cohort, longer CPB times and lower minimum CPB RSO2, temperature, and pH seem to play a more important role in SCT complications than the performance of ET.
Conclusions: This exploratory study merits confirmation in a larger randomized prospective study.
-
 NM-304 Image 1
NM-304 Image 1
Top










