
NM-202
Comparison of single shot caudal block with lumbar plexus block in children undergoing hip surgery: A retrospective study
1Wani T, 1Kadah K, 1Adam S, 2Veneziano G, 2Beltran R, 2Miller R, 2Tumin D, 2Tobias J
1King Fahad Medical City, Riyadh, NA, Saudi arabia; 2Nationwide Children's Hospital, Columbus, Ohio, United states
Background: Peripheral nerve blocks in children undergoing orthopedic procedures provide postoperative analgesia, reduce opioid consumption, decrease time to discharge, and minimize the exposure to general anesthesia. In patients undergoing hip surgery, lumbar plexus block may be advantageous compared to other blocks because it is the most reliable method of blocking the lateral femoral cutaneous, femoral, and obturator nerves. We evaluated whether lumbar plexus block offers advantages over caudal epidural blockade in children undergoing elective hip surgery by comparing perioperative and postoperative opioid consumption and postoperative pain scores.
Methods: Following Institutional Review Board approval, patients at King Fahad Medical City, aged 1 month to 17 years, who underwent elective hip surgery under general anesthesia with a single-shot lumbar plexus or caudal epidural block were identified using electronic medical records. The primary outcome evaluated was total dose of intraoperative and postoperative opioid within 24 hours after surgery. Opioid consumption was converted to oral morphine equivalents (ME) and assessed. Secondary outcomes included median pain scores at PACU admission, PACU discharge, and at 2-hour intervals for the first postoperative 24 hours. Variables were compared across anesthetic block using Wilcoxon rank-sum tests.
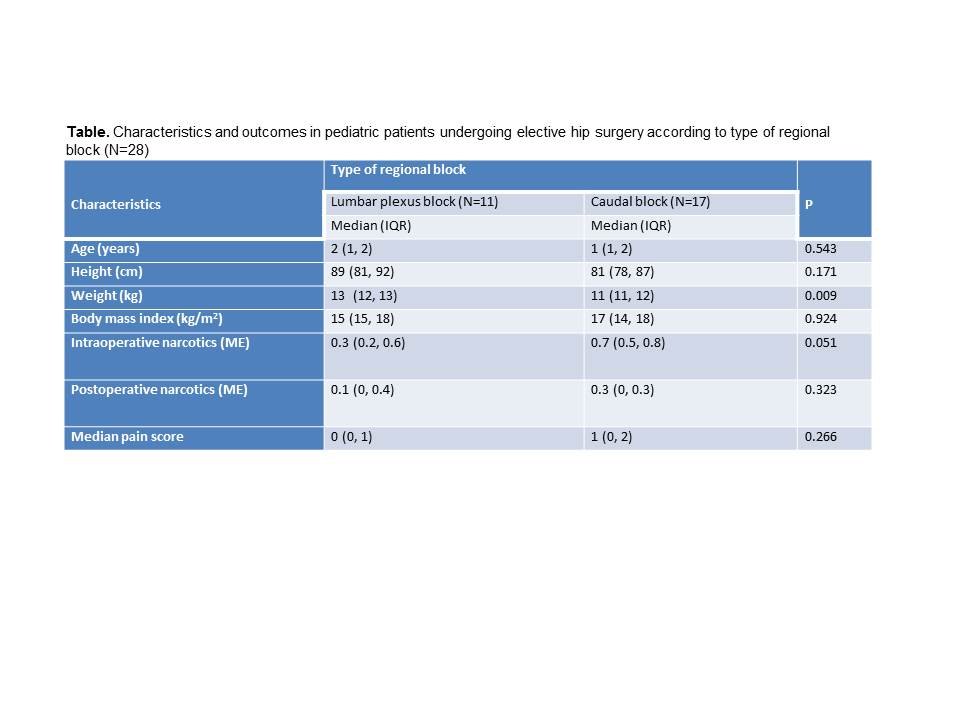
Results: Twenty-eight patients (median age 1 year; median height 82 cm; median weight 11 kg) were included in the study. Eleven received a lumbar plexus block and 17 received a caudal epidural block. Characteristics and outcomes are compared by anesthetic block in the Table. Intraoperative opioid use was 0.3 (interquartile range [IQR]: 0.2, 0.6) mg/kg of oral ME in the lumbar plexus group, compared to 0.7 (IQR: 0.5, 0.8) in the caudal block group (95% confidence interval [CI] of difference in medians: -0.007, 0.5; p=0.051). Postoperative (including PACU) opioid use was 0.1 (IQR: 0, 0.4) mg/kg of oral ME in the lumbar plexus group, compared to 0.3 (IQR: 0, 0.3) in the caudal group (95% CI of difference in medians: -0.1, 0.3; p=0.323). Over the first 24 hours after surgery, the median pain score in the lumbar plexus group was 0 (IQR: 0, 1), compared to 1 (IQR: 0, 2) in the caudal group (95% CI of difference in medians: 0, 1; p=0.266).
Discussion: Intraoperative opioid consumption in the caudal epidural block group was more than twice that in the lumbar plexus block group. There were no significant differences in postoperative opioid use or median pain scores according to type of regional block. A larger retrospective or a prospective study may be required to further define the postoperative efficacy between caudal epidural block and lumbar plexus block for postoperative analgesia.
References:
1. Ross AK, Eck JB, Tobias JD. Anesth Analg 2000; 91:16–26.
2. Grant C, Checketts M. Contin Educ Anaesth Crit Care Pain. 2008;8:56-61.
-
 NM-202 Image 1
NM-202 Image 1
Top










