
NM-349
Should we consider awake spinal anesthesia for surgery longer than 60 min in infants? Experience from the first 2 years of a spinal anesthesia program
Trifa M, Tumin D, Whitaker E, Jayanthi V, Tobias J
Nationwide Children's Hospital, Columbus, Ohio, United states
Background: To avoid potential risks of general anesthesia (GA), spinal anesthesia (SA) is increasingly being used in infants undergoing appropriate surgeries. An important limitation to SA is that it provides a relatively short duration of anesthesia, generally lasting less than 60 min. To clarify outcomes of SA for longer cases, we reviewed our experience with SA for long (≥ 60min) surgical procedures at a large tertiary care pediatric hospital. Our primary aim was to describe the incidence of success with SA.
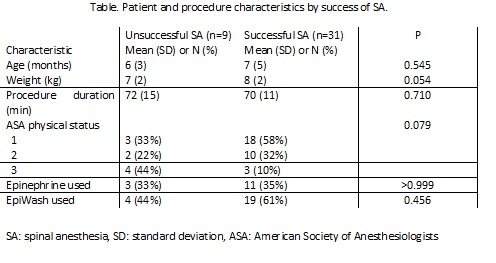
Methods: We retrospectively reviewed use of SA for surgical procedures (2015-17) lasting ≥60 min in children up to 3 years of age. All patients received bupivacaine 0.5% in a dose of 1 mg/kg (up to 7mg)±clonidine 1 µg/kg, and epinephrine or EpiWash. Success of SA was defined as successful lumbar puncture (LP) and SA initiation, without subsequent conversion to GA. Patient and procedure characteristics were compared according to SA success using unpaired t-tests for continuous data and Fisher’s exact tests for categorical data.
Results: Of 299 SA during the study period, 43 met inclusion criteria. Three patients were excluded because SA was associated with a caudal catheter insertion. Data from the remaining 40 male patients (age 7±4 months, weight 8±2 kg) were included in the analysis. Procedures included male genital, groin and multiple site surgeries in 24, 10 and 6 cases, respectively. Average procedure duration was 71±12 min (range: 60-111min). All but one patient received clonidine as an additive to bupivacaine. SA was successful in 31 cases (78%; 95% confidence interval: 61%,88%). Reasons for unsuccessful SA included inability to achieve LP (n=2), insufficient motor blockade (n=3), sustained cough causing extrusion of intestines through the hernia defect (n=1), failure to place a peripheral intravenous catheter in the leg (n=1), surgeon’s decision to convert to a laparoscopic procedure (n=1), and conversion to GA after 30 minutes (n=1). Six patients with successful SA required mild sedation using small doses of dexmedetomidine. Differences in procedure duration and patient characteristics were not statistically significant between successful and failed SA (Table). One patient developed a high SA, which was managed by positioning and oxygen administration, without conversion to GA. No complications or unanticipated admissions were deemed related to SA.
Discussion: SA is feasible for surgical procedures lasting longer than 60 minutes. Our success rate (78%) was similar to a previous report (84%) based on shorter procedures (mean time of 38 min). SA with bupivacaine0.5%, epinephrine and clonidine could be an alternative to GA in children undergoing appropriate surgery expected to last up to 120 min.
References:
1. Lambertz A et al. Pediatr Surg Int 2014;30:1069-73
2. Tirmizi H. Curr Opin Anaesthesiol 2015;28:333-8
3. Kokki H. Paediatr Anaesth 2012;22:56-64
4. Whitaker EE et al. J Pediatr Urol 2017;13:396-400
-
 NM-349 Image 1
NM-349 Image 1
Top










