
GA5-100
Opioid Sparing Effects of Medicinal Cannabis in a Child with Fibrodysplasia Ossificans Progressiva.
1Robbins R, 2Windsor R, 2Rampersad S
1Seattle Children’s Hospital, Seattle, WA, USA; 2University of Washington School of Medicine, Seattle Children's Hospital, Seattle, WA, USA
Introduction: A recent consensus report by the National Academy of Sciences concluded that there is substantial evidence that cannabis is an effective treatment for chronic pain in adults. 1 Currently, there is a paucity of quality studies looking into cannabis use in the treatment of chronic pain in children coupled with serious concerns about well-documented harms.2 While the AAP opposes legalization of cannabis because of potential harms to children, they nevertheless concede that “cannabis administration may be an option for children with life-limiting or severely debilitating conditions and for whom current therapies are inadequate.â€3
Fibrodysplasia ossificans progressiva (FOP) is a rare, debilitating disease characterized by progressive extra skeletal bone formation. Episodic flare-ups cause painful swelling, transforming skeletal muscle to bone. FOP is considered incurable; with treatment being primarily palliative.4 Here we present the successful use of medical cannabis for the treatment of chronic pain in a pediatric patient with FOP.
Presentation: An 11-year-old female with FOP was admitted to the ICU for acute on chronic respiratory failure secondary to a parainfluenza infection. The initial viral infection set off a series of painful FOP flares. While in the ICU, a hydromorphone PCA was initiated. Our pain service was consulted to manage her intractable pain.
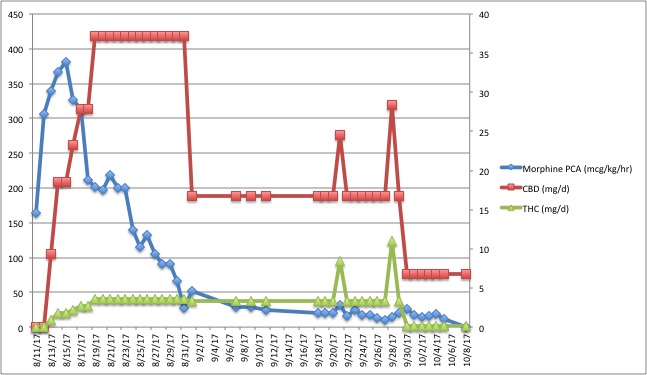
She escalated on her PCA to high-dose opioid requirements that remained refractory to opioid rotation and multimodal medications, including addition of steroidal and non-steroidal anti-inflammatories, methadone, benzodiazepines, pregabalin, clonidine, baclofen, and SSRI therapy. Following these trials, the patient’s family approached our pain and palliative care services about using medical cannabis to treat her pain. After meeting the state and hospital requirements for recommending cannabis use to a minor, our patient was started on a 10:1 CBD:THC tincture at 0.5mL once per day and gradually titrated upwards to effect (see Table 1). Over the course of eight weeks, she was able to discontinue her morphine PCA (after months of heavy use), wean her methadone, and reduce the number of adjunct pain medications and doses. Her pain remained improved despite ongoing FOP flares triggered by dental and abdominal procedures. Since initiating medicinal cannabis there have been no noticeable adverse psychoactive effects. The family reported improved mood and increased participation in physical and occupational therapy. The patient has ongoing pain in her shoulders, hips, jaw, and abdomen with stable reported pain scores. She has recently been transitioned off all intravenous opioid medications in hopes of facilitating her eventual discharge from the hospital.
Conclusion: This case demonstrates the successful use of medical cannabis for the treatment of chronic pain in a pediatric patient with FOP who was previously refractory to conventional therapies.
-
 GA5-100 Image 1
GA5-100 Image 1
Top










