
NM-265
Acute intraocular pressure variations at different stages of general anesthesia in children with retinoblastoma undergoing intravitreal injections of chemotherapy: a pilot study
1Mavarez A, 2Pruden B, 1Rodriguez L, 1Ripat C, 3Baux D, 4Cernichiaro-Espinosa L, 4Harbour W, 4Berrocal A, 5Tutiven J, 1Stein A
1University of Miami, Miami, Florida, USA; 2Thomas Jefferson University Hospital, Philadelphia, PA, USA; 3Philadelphia College of Osteopathic Medicine, Suwanee, GA, USA; 4Bascom Palmer Eye Institute, Miami, FL, USA; 5INSPIRE Cosmetic Surgery, Delray Beach, FL, USA
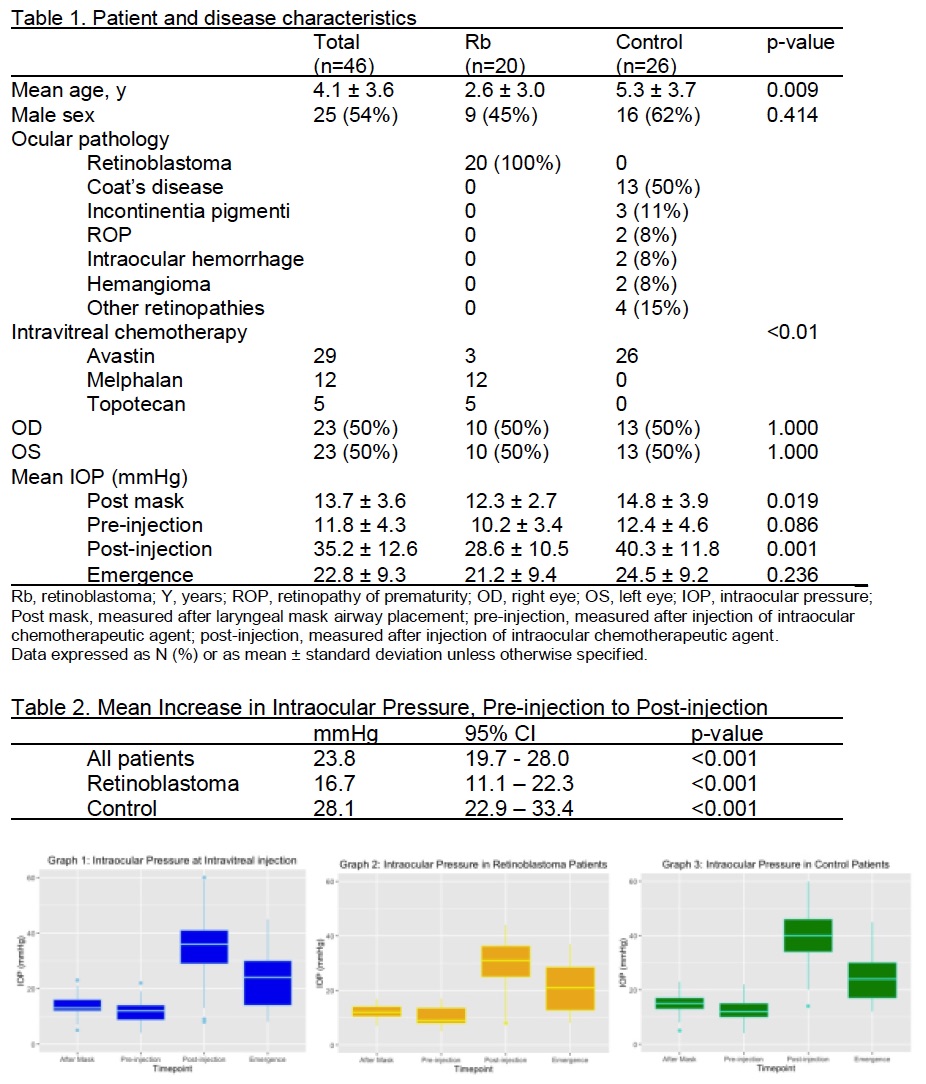
Introduction: Retinoblastoma (Rb) is the most common primary intraocular malignancy in children. Intravitreal injections of chemotherapy (iViC) are advocated as an adjuvant therapy to treat vitreous seeding as an effort to delay eye enucleation in addition to intra arterial chemoreduction1. There is theoretical risk of ischemic injury of the retina/optic nerve and extraocular tumor seeding from transient iViC rise in IOP2. Existing data on iViC on intraocular pressure (IOP) in anesthetized children is lacking and controlled studies are limited. Physiologic and pharmacologic factors during general anesthesia (GA) can affect IOP3. The aim of the study was to compare IOP changes in Rb and nonRb eyes that received iViC under GA. We hypothesized that Rb eyes would have higher IOPs than nonRb eyes after iViC and proposed non invasive anesthetic measures to reduce IOP. Methods: IRB-approved retrospective study of 30 children (<18 yo) 46 eyes, who received iViC under GA over a 2-year period, from Feb2015 to Nov2017. Patients underwent inhalational induction and maintenance via laryngeal mask airway with Sevoflurane/O2/Air. IOP was measured using a Tono-pen (Reichert, Inc. Buffalo, NY) instrument at 4 peri-anesthetic times: (1) post-induction, (2) pre-iViC, (3) post-iViC and (4) prior emergence. iViC agents included bevacizumab (1.25mg/0.05ml), melphalan (20μg/0.05ml) and topotecan (7.5μg/0.03ml).Continuous variables were compared with Student’s two sampler-test and Pearson’s chi-square test or Fisher’s exact test for categorical variables. Results: Patient demographics were distributed even in sex and OD/OS. NonRb group was older than Rb group, mean age 2.6 vs 5.3 years, p=0.009 (Table1). All IOP measures showed a post induction drop followed by an overall increase post-iViC (Graph1). The nonRb group had greater IOPs at all 4 times of the anesthetic over the Rb group (Graph3&4) with a mean IOP increase of 28.1 vs 16.7 mmHg, p<0.001(Table 2). Discussion: The hypothesis that Rb eyes would have increased IOP after iViC relative to nonRb eye due to Rb tumor load was not proven. Further studies need to be done to determine if these acute elevations in IOP are of clinical significance. If the case, adjuvant non invasive anesthetic interventions are suggested. Conclusion: iViC for Rb is associated with transient elevations in IOP which were not significantly higher than in its use in pediatric nonRb retinal pathology, making the risk of glaucoma and extra ocular tumor seeding less likely. The amount of fluid injected was related to the IOP increase. References: 1Munier et al. Intravitreal chemotherapy for vitreous seeding in retinoblastoma. Saudi J Ophthal 2013;27,147-150 2Karl et al. Intraocular pressure changes following intravitreal melphalan and topotecan for the treatment of retinoblastoma with vitreous seeding. J Pediatr Ophthal Strab 2017;54,185-190 3Mikel et al. Effect of intraocular pressure measurements in children. S Ophthal 2017;62,648-658
-
 NM-265 Image 1
NM-265 Image 1
Top










