
GAP-108
Lack of tachycardic response to hypotension in a child with perihepatic hematoma: Case Report
Chu K, Costandi A
Children's Hospital Los Angeles, Los Angeles, California, United states of america
CASE:
A 21-month old female presented with jaundice, elevated LFTs, elevated INR 1.6 requiring urgent percutaneous liver biopsy. Anesthesia was induced with propofol, maintained with sevoflurane, and airway secured with LMA. Patient received FFP during the procedure, remained hemodynamically stable, and extubated deep at the conclusion of surgery. 0.5mcg/kg of dexmedetomidine was administered to help her lie flat in the recovery room for observation.
One hour later in the PACU, she became hypotensive without significant change in pulse. Blood pressure improved with fluid bolus, raising concerns for bleeding. Abdominal ultrasound revealed a large perihepatic hematoma (Image 1). Hemoglobin dropped to 5.6 gm/dl for which she was transfused with 20 ml/kg PRBCs, 20ml/kg FFP, 1 unit of platelets, and then transferred to the ICU for monitoring.
DISCUSSION:
Dexmedetomidine is an alpha2-adrenergic agonist that produces sedation and anxiolysis. Two common side effects include hypotension and bradycardia. Although there is no literature on elimination half-life of dexmedetomidine in patients with liver failure, it is recommended to decrease the dose in patients with hepatic dysfunction1.
The presence of tachycardia is often considered to be an important sign in the initial diagnosis of hemorrhagic shock. Elevation of heart rate in response to hypotension is a mechanism for the body to maintain cardiac output. Lack of tachycardia to hemorrhagic hypotension has been recorded in some adult trauma patients and was associated with increased mortality2.
This is the first case in literature describing an absent tachycardic reflex in response to hemorrhagic hypotension in the pediatric population. It highlights a safety issue for pediatric anesthesiologists given that cardiac output is largely heart rate dependent in this age group. The heart rate did not change by more than 10% of the baseline despite profound hypotension. The relative bradycardia may have been due to a parasympathetic reflex mediated by the vagus nerve in response to hemoperitoneum3 or from the dexmedetomidine, with its delayed elimination in children, especially those with impaired hepatic function.
CONCLUSION:
The diagnosis of hemorrhagic shock should be considered in patients at high risk for bleeding, especially those who have received dexmedetomidine, even in the absence of tachycardia.
REFERENCES
1. Precedex [package insert]. Hospira, Inc.; October 2008. www.precedex.com
2. Ley E, Salim A, Kohanzadeh S. Relative Bradycardia in Hypotensive Trauma Patients: A Reappraisal. Journal of Trauma-Injury Infection & Critical Care: November 2009 - Volume 67 - Issue 5 - pp 1051-1054.
3. Oberg P, Thoren P. Increased activity in vagal cardiac afferents correlated to the appearance of reflex bradycardia during severe haemorrhage in cats. Acta Physiol Scand 1970;80: 22A-23A.
-
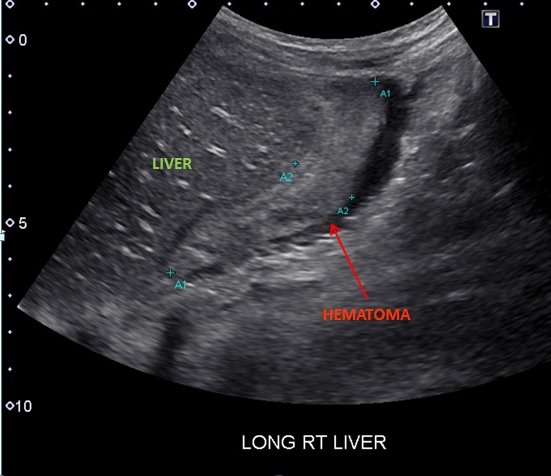 GAP-108 Image 1
GAP-108 Image 1
Top










