
NM-252
3D Printing Provides Organization, Standardization and Simplification of Access to Emergency Anesthesia Medications in the Pediatric Operating Rooms: A Quality Improvement Initiative
1Scholl R, 2Elbert K, 1Taicher B
1Duke University Medical Center, Durham, NC, USA; 2Duke University, Durham, NC, USA
Introduction: During an emergency in the pediatric operating rooms (ORs), immediate access to medications is essential to the anesthesia team. Delays in administration during an emergency can result in untoward patient outcomes. In the pediatric ORs at Duke University Hospital, there is a division consensus on type and location of emergency medications for every pediatric anesthetic. This sought to standardize these medications so that any anesthesia provider responding to an emergency could immediately find them. After discussing a critical event that occurred because of misappropriation and misplacement of emergency medications, we decided to use 3D technology to improve responsiveness to pediatric anesthesia emergencies.
Methods: An unannounced audit of the pediatric ORs was conducted to identify deviance from this consensus. Although education on these expectations are provided for all pediatric CRNA’s and anesthesia residents, the audit found variability in both the types and location of medications prepared. Using Qualtrics, a survey was administered to both pediatric CRNAs as well as residents to assess current practice. Finally, we designed a 3D-printed model that would integrate with the anesthesia workspace and provide all team members a simplified solution for organizing emergency medications.
Results: The survey was administered to 27 anesthesia providers. All providers answered that atropine, succinylcholine and epinephrine should be immediately available and readily located. However, only 55% were aware of the divisional consensus on the locations of these emergency drugs. Of this 55%, 80% identified the correct IV epinephrine location and 40% identified the correct IM succinylcholine and IM atropine location. For those surveyed who were unaware of the divisional consensus, inconsistencies existed on their preferred locations for these medications. Of note, it was indicated that providers place epinephrine in 4 disparate locations by providers. Although 52% answered that they ‘never struggle’ with maintaining organization of their workspace, 80% answered that they would be receptive to utilizing a device that organizes, standardizes, and simplifies access to emergency anesthesia medications.
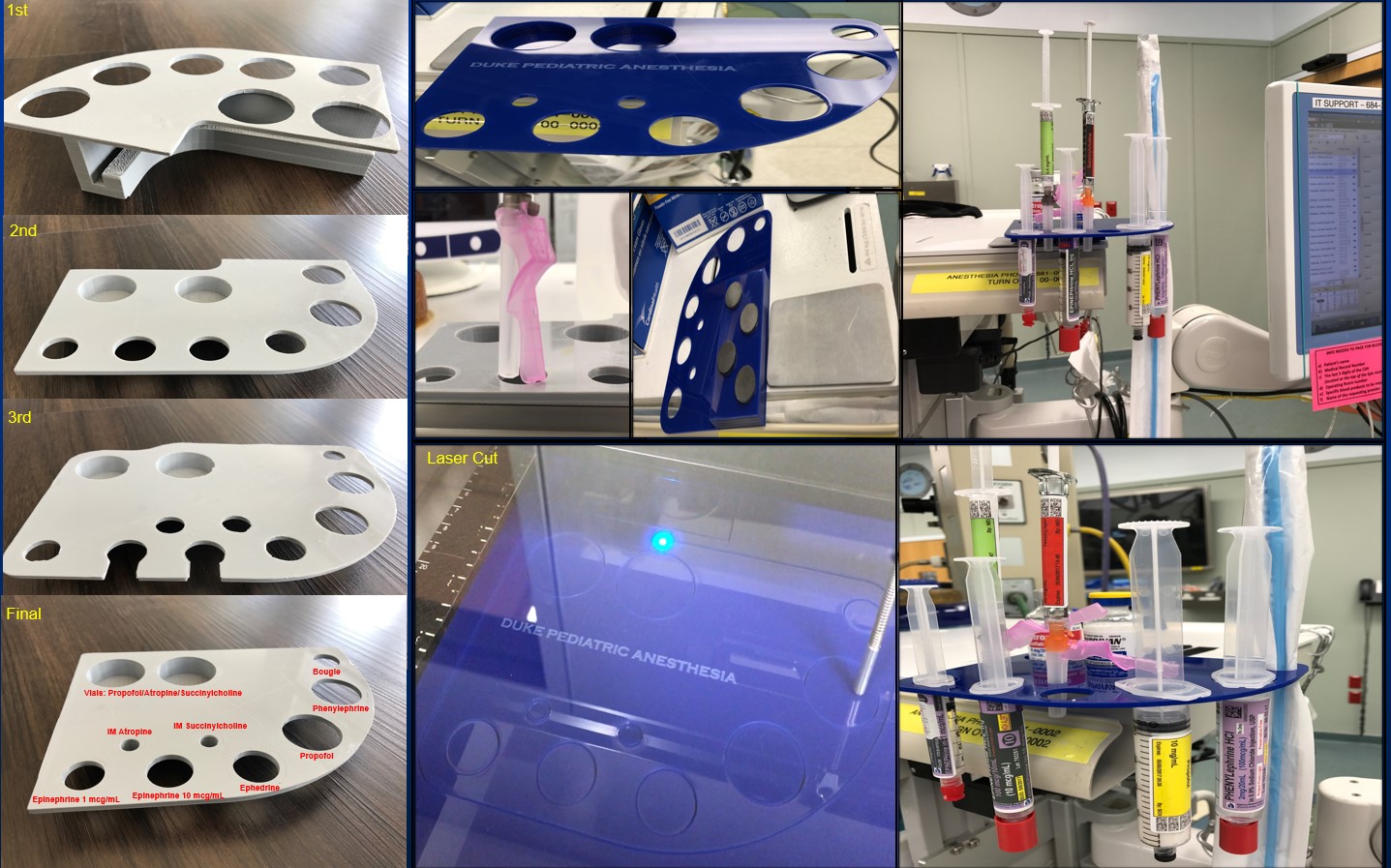
Over 7 months, multiple 3D models were printed in the Duke Innovation Co-Lab. Each model is designed to hold IM succinylcholine, IM atropine, both 1 mcg/ml and 10 mcg/ml concentrations of epinephrine, a propofol syringe, 2 vials of unopened medications, and an intubating stylet. Each iteration of the model improved the functionality of the device. The device is secured magnetically on top of the anesthesia machine. After division approval and anesthesia provider education it was deployed in all pediatric ORs.
Conclusion: Creating a device using 3D printing that is simple to use by all providers and reliably secures and locates pediatric emergency drugs can improve the shared mental model by all team members.
-
 NM-252 Image 1
NM-252 Image 1
Top










