
NM-303
Eliminating routine preoperative laboratory studies in outpatient pediatric cardiothoracic surgery patients: a quality improvement study
Jones S, Machovec K, Ames W, Homi H, Poisson J, Bandarencko N, Lodge A, Turek J, Jooste E
Duke University Medical Center, Durham, NC, United states of america
Introduction: Preoperative laboratory testing is standard of care for pediatric patients scheduled for cardiac surgery. However, clinical studies examining the need for routine preoperative testing in pediatric patients undergoing elective noncardiac surgery indicate that tests are expensive and largely unnecessary.1-2 More recently, Nieto et al evaluated the utility and expense of routine preoperative laboratory studies for elective pediatric cardiac procedures and concluded that these tests are expensive and do not influence medical decision making.3 Furthermore, the effect of multiple sticks on available venous access, anxiety experienced by the patient as a result of blood draws, and resources spent by the family and the hospital prior to the day of surgery have not been considered.
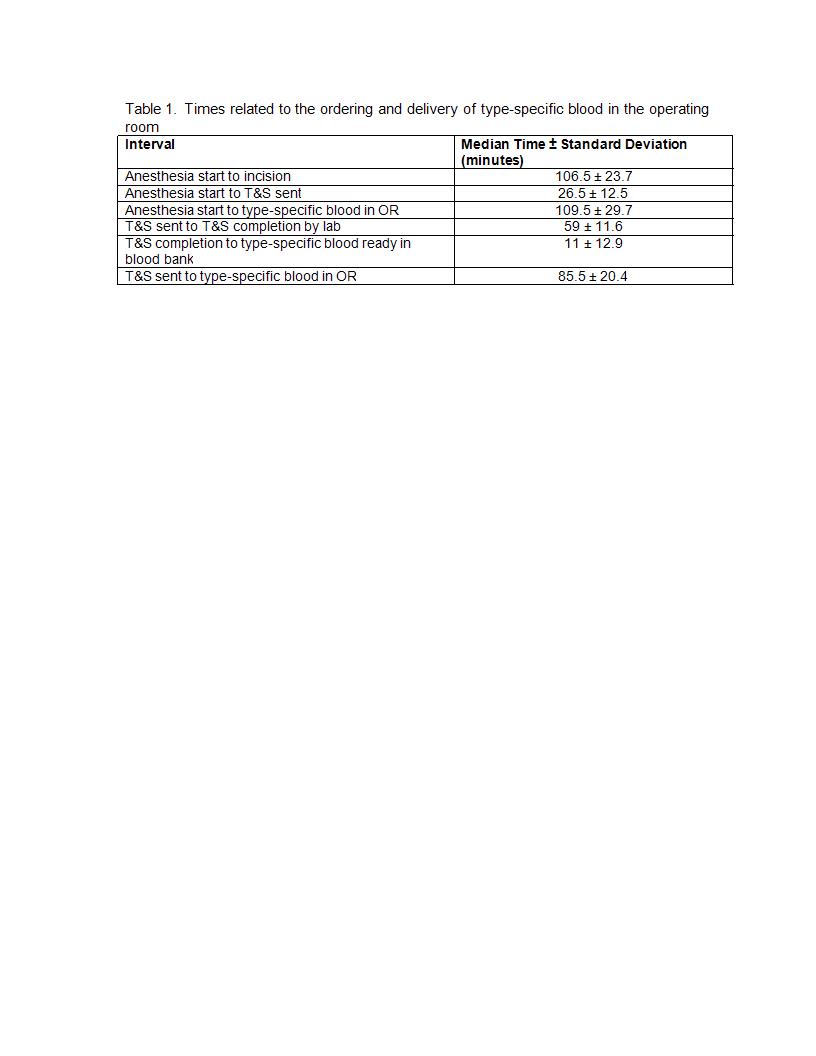
Methods: We eliminated all preoperative blood-based lab testing for pediatric outpatients scheduled for elective cardiac surgery. We obtained a post-induction, pre-incision type and screen (T&S) and arterial blood gas (ABG) that includes a hematocrit. We prospectively monitored the time required to obtain type-specific blood in the operating room (OR). Additional time points monitored included start of anesthesia care, time that T&S was sent, time that T&S resulted in the electronic medical record, time that type-specific blood was ready in Transfusion Services, time that type-specific blood was delivered to the OR, and incision time. If type-specific blood was not ready prior to incision, one unit of O negative blood was brought to the OR prior to incision.
Results: Over a five-week period, 17 out of 30 patients presented as outpatients for elective procedures. Five patients (ages 14 to 25 years) had laboratory studies drawn preoperatively. Eight of 12 cases requested that type O negative blood be brought to the OR as type-specific blood was not ready prior to incision. Four cases had type-specific blood in the room at the time of incision. Incision time was delayed by approximately four minutes in one case to wait for type-specific blood to arrive in the room (Table 1).
Discussion: Elimination of all preoperative laboratory studies, including a T&S, is feasible with collaboration of the whole congenital cardiac surgery team. There are significant benefits to this practice without introducing significant risk. The use of O negative blood is safe as the incidence of antibodies is exceedingly rare in this patient population and ordering of one unit of O negative blood does not deplete this resource. Continued revision of hospital processes and this protocol are underway.
References
1. American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2002;96:485-96.
2. Meneghini L, Zadra N, Zanete G, Baiocchi M, Giusti F. Paediatr Anaesth. 1998;8:11-5.
3. Nieto RM, De León LE, Trujillo Diaz D, Krauklis KA, Fraser CD. J Thorac Cardiovasc Surg. 2017;153:678-85.
-
 NM-303 Image 1
NM-303 Image 1
Top










