
NM-293
Effect of Dexmedetomidine on Pacemaker Function During Cardiac Surgery
King A, Tumin D, Naguib A, Winch P, Kertesz N, Tobias J
Nationwide Children's Hospital, Columbus, Ohio, USA
Introduction:Dexmedetomidine is frequently used in anesthesia to provide effective sedation, reduce emergence delirium, and potentiate opioid analgesia. In the congenital cardiac population, it has been shown to accelerate extubation, blunt the surgical stress response and to improve postoperative pain control. Despite these benefits, rare anecdotal reports suggest that dexmedetomidine may adversely affect pacemaker function by limiting the ability of the impulse to elicit an atrial or ventricular response, and therefore requiring a stronger impulse to be used. To address this possibility, we prospectively compared dexmedetomidine dosing to intraoperative pacemaker function during congenital cardiac surgery.
Methods: After IRB approval, we prospectively enrolled children undergoing cardiac surgery with cardiopulmonary bypass and placement of temporary pacemaker leads. No changes were made to intraoperative care. Following the insertion of the temporary pacing wires , we recorded the amplitude required for atrial or ventricular capture, and total dexmedetomidine dose received.A Spearman correlation coefficient was used to determine whether amplitudes were higher when larger doses of dexmedetomidine were used.
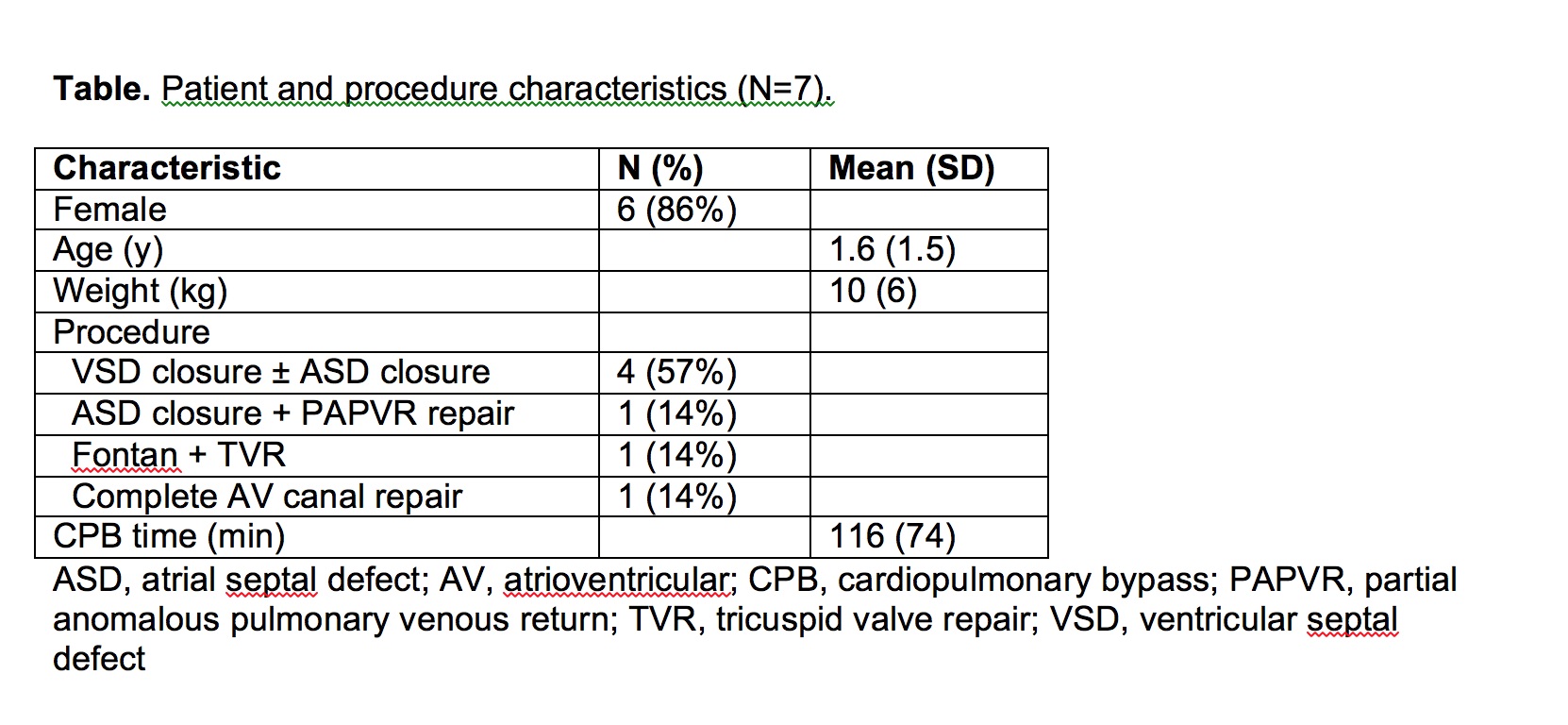
Results: One boy and 6 girls, ages 5 months to 4 years, have been enrolled in the study to date. Patient demographics and procedure characteristics are summarized in the Table. All patients received 0.5 µg/kg/hr dexmedetomidine infusion with no supplemental boluses. At the intraoperative evaluation all patients were either still receiving dexmedetomidine (n=3) or had dexmedetomidine discontinued <20 minutes prior (n=4). Total dexmedetomidine dose averaged 1.8 ± 0.9 µg/kg. Three of the children were in sinus rhythm following pacing wire insertion but were briefly paced for the purposes of the study. The other 4 children had bradyarrhythmias including AV-block, sinus bradycardia and a junctional rhythm and required pacing in the postoperative period. One out of the 7 children had atrial pacing wires inserted only while the others had ventricular pacing wires only. The amplitude required to elicit atrial capture and ventricular was 3.5 mA) and (1.2 ± 0.4 mA) respectively and this did not correlate with the dexmedetomidine dose administered. (rho=-0.43, p=0.397).
Discussion: In this prospective study of temporary pacemaker function during pediatric cardiac surgery, we did not find a correlation between the intraoperative dose of dexmedetomidine administered and the requirement for a greater amplitude in order to elicit ventricular capture. Further prospective enrollment of a comparison cohort not receiving postoperative dexmedetomidine may confirm the lack of association between dexmedetomidine and pacemaker function in these patients.
References
1. Pediatr Cardiol 2011;32:1075-1087
2. Pediatr Crit Care Med 2013;14:481-490
3. Pediatr Cardiol 2013;34:779-785
4. Crit Care Med 2011;39:187-189
-
 NM-293 Image 1
NM-293 Image 1
Top










