
NM-251
Predicted obstructive sleep apnea on a short caregiver questionnaire and post-anesthesia care unit outcomes
Raman V, Jatana K, Splaingard M, Tumin D, Tobias J
Nationwide Children's Hospital, Columbus, OH, USA
Introduction: Screening for obstructive sleep apnea (OSA) may help avoid perioperative morbidity and mortality. However, few children undergo definitive testing for OSA using polysomnography (PSG). Our group created a short questionnaire tool predicting OSA (apnea-hypopnea index >5) on PSG, We found that both diagnosed and predicted OSA correlated with increased need for supplemental O2 in the PACU. In this study, we evaluate the association between predicted OSA and PACU outcomes in a large, prospective cohort.
Methods: IRB obtained. Patients, from 3-18 years of age, ASA status 1-3, were prospectively enrolled on the day of surgery. Caregivers completed a 6-item questionnaire on OSA-related symptoms (e.g, snoring), and scores ≥ 2 of 6 were classified as “predicted OSA.†PACU outcomes were queried from the electronic medical record. These specifically included supplemental O2 requirement and prolonged length of stay (LOS >1 hour). Outcomes were compared using unpaired t-test/.
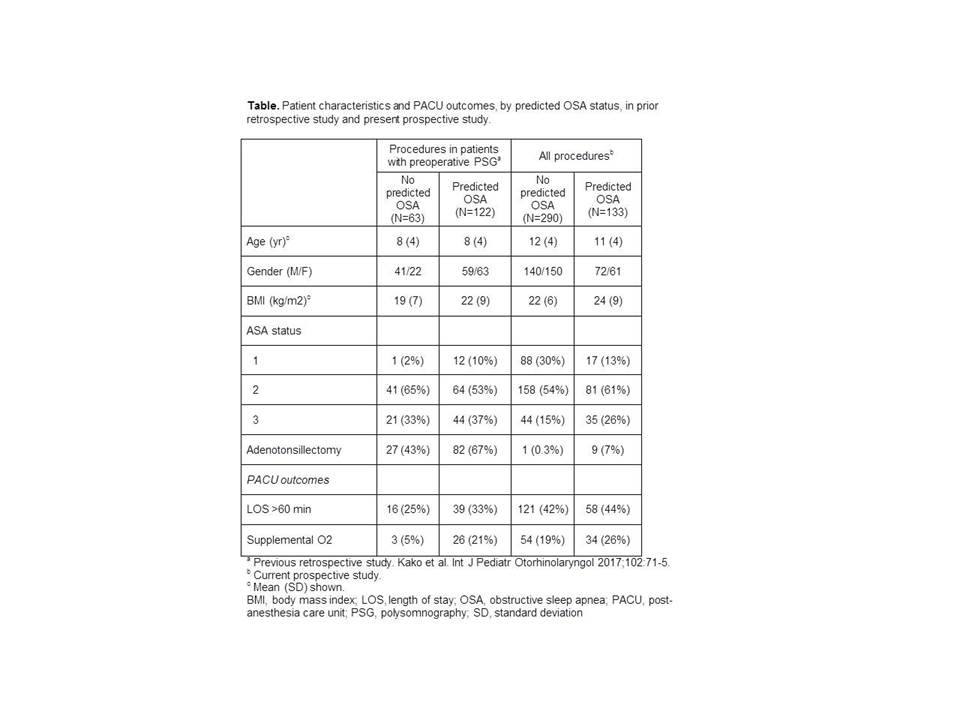
Results: We enrolled 212 boys and 211 girls to date, age 12 ± 4 years. Patient characteristics and PACU outcomes are compared to our retrospective study in the Table. The difference in supplemental O2 requirement in PACU between children with predicted OSA (26%) and children without predicted OSA (19%) did not reach statistical significance (95% CI of difference: -1%, +16%; p=0.102), and was smaller than the difference of 16% found in the previous study (Table). However, on conditional power analysis, the study had 74% power to confirm the smaller difference in supplemental O2 requirement at p<0.05 with the planned total enrollment of 1000 patients. Prolonged PACU LOS was not significantly more likely among children with predicted OSA (44%) compared to those without predicted OSA (42%; 95% CI of difference: -8%, 12%; p=0.716).
Discussion: Despiterisks related to OSA in the perioperative period, the association between OSA and postoperative outcomes remains unclear. We used a questionnaire tool developed to predict OSA on PSG to prospectively evaluate its association with PACU outcomes. Compared to a previous retrospective analysis limited to children who had undergone PSG, this prospective study found a smaller difference in supplemental O2 requirement in PACU according to predicted OSA. Nevertheless, our results suggest that undiagnosed OSA may pose a risk of respiratory complications in PACU after procedures unrelated to OSA symptoms.
References
1. Tait AR, Voepel-Lewis T, Christensen R, O’Brien LM. Paediatr Anaesth 2013;23:510-6.
2. Raman VT, Splaingard M, Tumin D, Rice J, Jatana KR, Tobias JD. Paediatr Anaesth 2016;26:655-664.
3. Kako H, Tripi J, Walia H, Tumin D, Splaingard M, Jatana KR, Tobias JD, Raman VT. Int J Pediatr Otorhinolaryngol 2017;102:71-5.
-
 NM-251 Image 1
NM-251 Image 1
Top










