
GA3-73
Intracuff pressure during one-lung ventilation in infants and children
1Hakim M, 2Hakim M, 3King A, 4Kamata M, 5Tumin D, 5Krishnna S, 5Naguib A, 5Tobias J
1Natinwide Children's Hospital, Columbus, Ohio, USA; 2Montefiore Medical Centre, Bronx, New york, USA; 3Nationwide children's Hospital, Columbus, Ohio, USA; 4Chlidrens Medical Centre, Saitama, Shintoshin, Japan; 5Nationwide Children's Hospital, Columbus, Ohio, USA
Introduction: Several techniques have been described for one-lung ventilation (OLV) in pediatric thoracic surgeries, including a Univentâ„¢ endotracheal tube (ETT), double-lumen ETT (DLT), bronchial blocker, and selective endobronchial intubation. All of these devices use a cuff inflated in the bronchus to selectively ventilate one of the lungs. Excessive intracuff pressure (IP) may lead to damage to the bronchus or cuff rupture. Despite this risk, bronchial IP is not routinely measured, and the bronchial cuff is usually inflated during bronchoscopic visualization of the balloon until the bronchus appears to be occluded. To quantify the risk posed by over-inflation of the cuff used for OLV, this study describes IP during OLV in infants and children.
Methods: After Institutional Review Board approval, we prospectively enrolled children ≤18 years of age requiring OLV for thoracic surgery. Premedication, induction, and maintenance of anesthesia was performed according to standard practice, with the exception of measuring the IP with a Cufflator. After cuff inflation, ventilation parameters were set to maintain normocarbia with a tidal volume of 7-10 mL/kg and an inspired oxygen concentration of 40-50% in air and oxygen. IP was measured after positioning the patient, inflating the cuff, and initiating OLV. IP greater than 30 cmH2O was considered excessive, and study data were compared according to the type of OLV device.
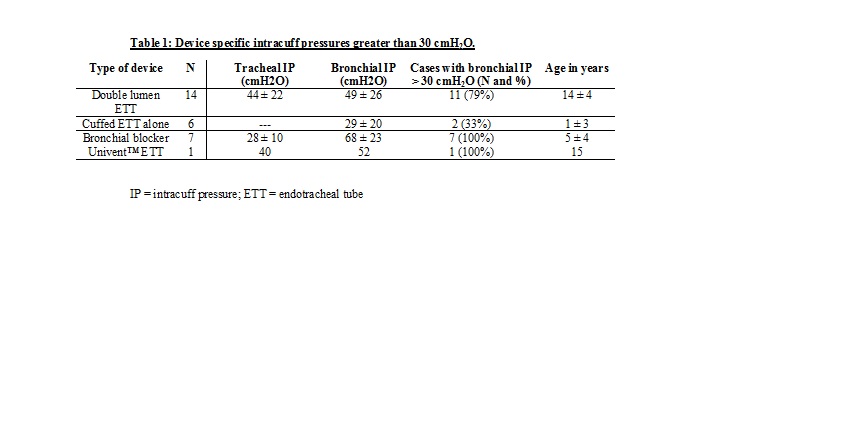
Results: The study cohort included 28 patients age 9 ± 7 years (range: 5 months-18 years), with an average weight of 40 ± 32 kg (range: 5 to 131 kg). There were 13 cases of left lung isolation and 15 cases of right lung isolation. Procedures included wedge resection (9), paraspinal mass resection (4), lobectomy (3) and others (12). A double lumen ETT, cuffed ETT alone (mainstem intubation), bronchial blocker, and the Univent™ ETT were used in 14, 6, 7, and 1 patients respectively (Table). Average tracheal and bronchial IP were 39 ± 20 and 50 ± 26 cm H2O respectively. The tracheal and bronchial IP exceeded 30 cmH2O in 13 of 20 patients (65%) and 21 of 28 patients (75%), respectively. In one case, air was removed from the cuff due to overinflation, and in another case, a larger ETT was used. No other maneuvers were undertaken to reduce IP, and no complications related to excess IP were noted.
Discussion: Intracuff pressures were high in most children undergoing OLV, regardless of the device used. Given that cuffs on OLV devices lack the high-volume, low-pressure design of polyurethane cuffs used in standard cuffed ETTs, there may be a risk of damage to the bronchus. Continuous monitoring of IP may be indicated during OLV to address this risk.
Conclusion: Intracuff pressure was elevated in children undergoing OLV irrespective of the tube used.
References
1. Curr Opin Anesthesiol 2001;14:77-85.
2. Inter J Pediatr Otorhinolaryngol 2013;77:1135-18.
3. Pediatr Anesth 2014;24:999-1004.
-
 GA3-73 Image 1
GA3-73 Image 1
Top










