
GA5-102
Robotic dose-splitting as a novel intervention to optimize operating room medication utilization in a pediatric hospital
Sanders K, Karnwal A, Lau J
Children's Hospital of Los Angeles, Los Angeles, CA, USA
Robotic dose-splitting as a novel intervention to optimize operating room medication utilization in a pediatric hospital
Kyle Sanders M.D., Abhishek Karnwal M.D., and Jennifer Lau M.D.
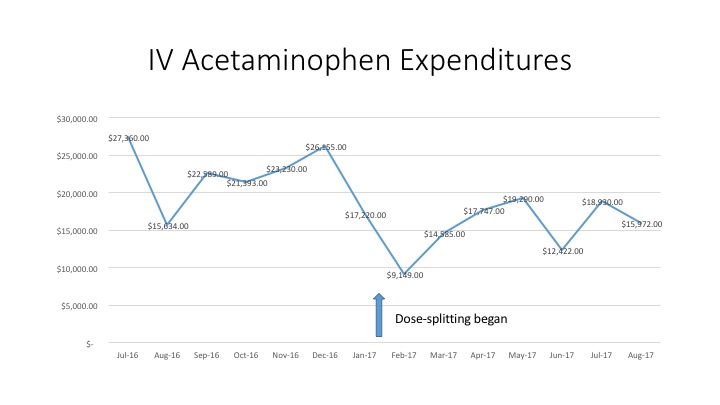
Background: Operating room (OR) costs comprise 40% of all hospital expenditures and are a prime target for improved efficiency2. Anesthetic drug waste, one example of operating room inefficiency, represents nearly 30% of total anesthetic drug expenditures, due primarily to the disposal of full or partially full syringes1. Concerns about drug sterility and patient safety have lead regulatory bodies to discourage the practice of “dose-splittingâ€, using a single vial of medication for multiple patients, in the OR.  This limitation has the potential to increase waste, particularly in pediatric hospitals where often only a small fraction of a vial is needed per patient. To address these concerns, our ORs instituted a practice of robotic dose-splitting of intravenous (IV) acetaminophen (APAP) vials (1000 mg/100 mL) into syringes of 20 mL/200 mg each.  This technique was performed in the satellite pharmacy, satisfying sterility requirements.  We aim to investigate the impact of this change on IV APAP expenditures and waste in the OR.
Methods: This was a retrospective analysis of IV APAP usage at Children’s Hospital Los Angeles (CHLA).  Data was obtained from pharmacy billing records and drug purchase invoices for the period Jan 2016-Oct 2017. The dose-splitting program was initiated in Jan 2017. Â
Results: Hospital expenditures for IV APAP decreased by 32.4% in the 6 months following the intervention compared to the 6 months prior, while total doses given in the OR decreased by 9.2%. Between Jan 2017-Aug 2017, IV APAP doses administered in the OR represented 41.8% of the total hospital use at CHLA. Total spending on IV APAP for that time period was $125,366, yielding an estimated $52,402 spent on IV APAP in the ORs alone.
Discussion: Our results suggest robotic dose-splitting of anesthetic medications may lower costs and reduce waste while improving compliance with Joint Commission standards. Â Exact amounts of IV APAP waste could not be directly measured retrospectively due to documentation limitations. A portion of the observed cost savings can be attributed to the 9% decrease in usage, but the magnitude of the reduction in expenditures suggests a decrease in drug waste. The principle of dose-splitting is broadly applicable to many drugs used in the OR environment.
Conclusion: Robotic dose-splitting may reduce OR drug waste, save costs, and improve compliance with Joint Commission guidelines.
References:
1. Gillerman RG, Browning RA. Drug use inefficiency: A hidden source of wasted health care dollars. Anesth Analg. 2000;91:921–4
2. Macario A, et al. Where are the costs in perioperative care? Analysis of hospital costs and charges for inpatient surgical care. Anesthesiology. 1995;83:1138–44.
-
 GA5-102 Image 1
GA5-102 Image 1
Top










