
NM-273
Anesthetic management of a rare case of endobronchial granuloma in a toddler.
1Baronos S, 2Pryjdun O, 2Chon B
1New York Presbyterian Brooklyn Methodist Hospital, BROOKLYN, NY, United states; 2Westchester Medical Center, Valhalla, NY, USA
Introduction
Non-tuberculous mycobacteria are ubiquitous and are responsible for cervical lymphadenopathy in children.1 Intrathoracic and endobronchial disease due to non-tuberculous mycobacteria is exceedingly rare in immunocompetent children.
We present a case of a 1 year old patient with multiple mediastinal masses that presented for excision of an endobronchial lesion.
Case description
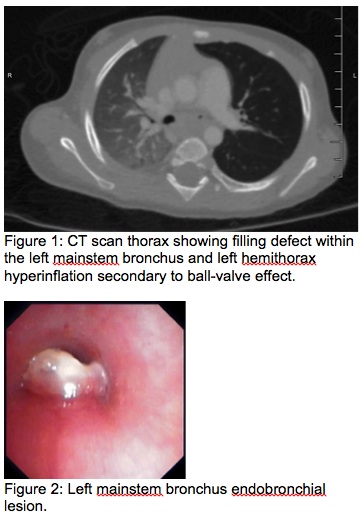
A 1-year-old healthy boy presented with 7 week history of labored breathing, expiratory stridor and fever. MRI showed middle mediastinal masses. Serologies and BAL were negative.
In the OR, patient was placed supine, ASA monitors affixed and IV midazolam and dexmedetomidine titrated. Sevoflurane was used for induction and spontaneous ventilation maintained. LMA was placed and propofol infusion started prior to the bronchoscopy where the left mainstem bronchus lesion was resected. Pathology report showed necrotizing granuloma.
Discussion
Mediastinal masses were later excised and pathology showed granulomas due to mycobacterium avium complex (MAC). MAC usually causes invasive disease in immunocompromised patients. In healthy pediatric patients younger than 5 years, there is an increased incidence of MAC infections, usually causing cervical lymphadenopathy.2 The finding of an endobronchial granulomatous lesion associated with mediastinal MAC lymphadenopathy in an immunocompetent toddler is exceedingly rare and is likely related to inhalation of contaminated materials.1
Treatment options depend on the severity of the disease. Most patients are treated with macrolides, ethambutol, and rifampin, however, there are reports of clinical improvement with only surgical excision of the infected tissue.1
A thorough preoperative assessment is important to mitigate the possibility of airway occlusion. Imaging may suggest the degree of compression. While flow-volume loops is the gold standard, it can only be done in older, cooperative child.
Relaxation of the tracheobronchial smooth muscles under anesthesia increases the risk of airway occlusion and paralytics should be avoided. Induction and maintenance of anesthesia should focus on preserving spontaneous respirations. This is particularly important in children since they have smaller airways and limited cardiopulmonary reserve.3
Conclusion
GA for patients with endobronchial and/or mediastinal masses can be challenging and requires the highest level of preparedness. Spontaneous respirations should be maintained to minimize airway occlusion.
Reference:
1. Freeman AF, Olivier KN, Rubio TT, et al. Intrathoracic Nontuberculous Mycobacterial Infections in Otherwise Healthy Children. Pediatric pulmonology. 2009;44(11):1051-1056
2. Nolt D, Michaels MG, Wald ER (2003) Intrathoracic disease from nontuberculous mycobacteria in children: two cases and a review of the literature. Pediatrics 112: e434
3. Hammer GB. Anaesthetic management for the child with a mediastinal mass. Paediatr Anaesth. 2004;14:95–7
-
 NM-273 Image 1
NM-273 Image 1
Top










