
GA4-85
MASSIVE TRANSFUSION DURING EMERGENCY EX-UTERO INTRAPARTUM TREATMENT PROCEDURE FOR DELIVERY OF INFANT WITH CONGENITAL INFANTILE FIBROSARCOMA
Oster A, George P, Moore R, Fehr J, Reina E, Cox T
Washington University School of Medicine, Saint Louis, MO, USA
INTRODUCTION:
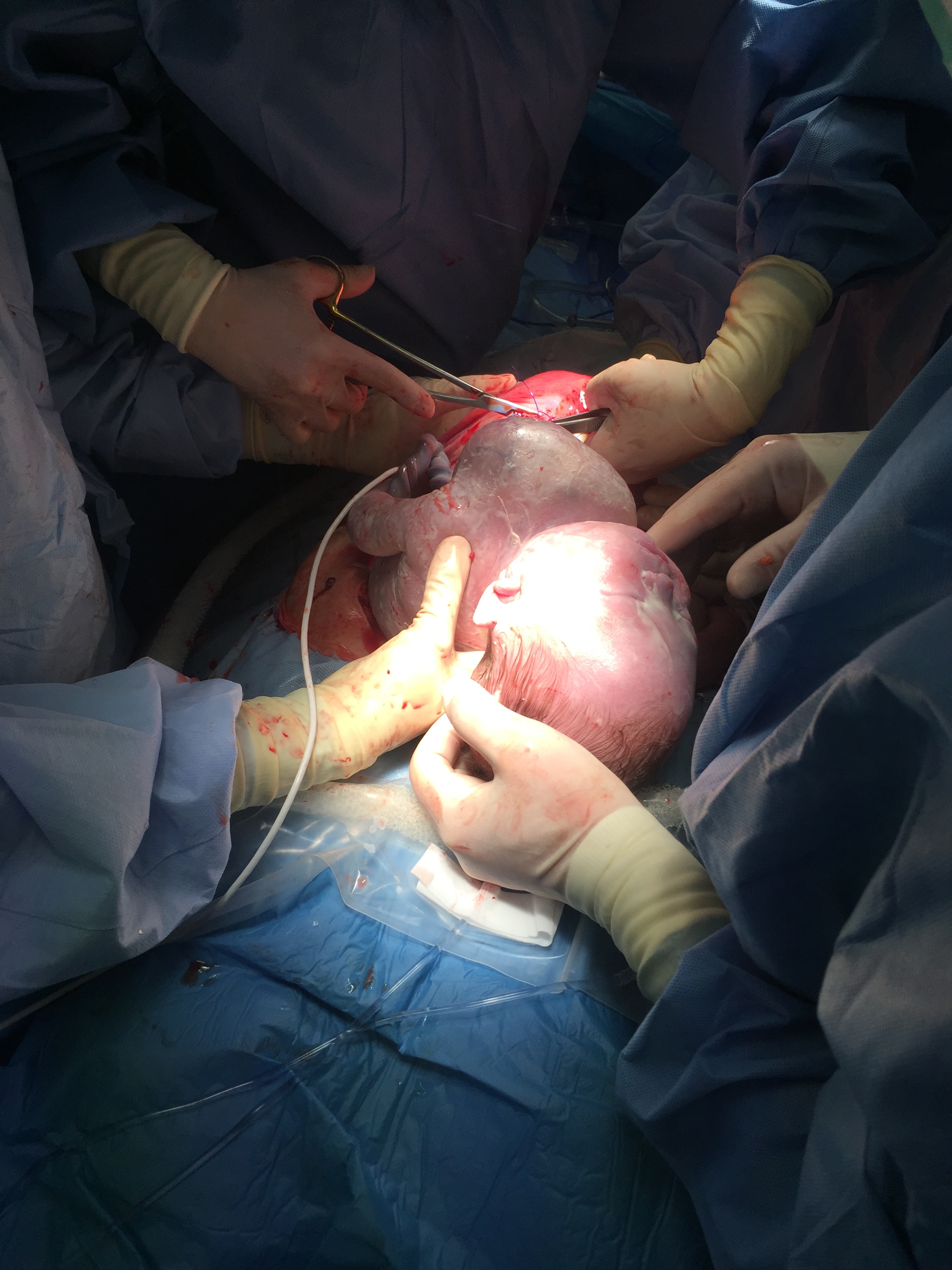
Infantile Fibrosarcoma (IFS) is a rare tumor accounting for 1% of all childhood cancers. These highly vascular tumors are discovered at birth and commonly involve limbs and seldom the head, neck and trunk. We present the case of a giant anterior cervical mass with an intrathoracic extension that progressed to hydrops and mandated an emergent EXIT (ex-utero intrapartum treatment procedure). This was successfully managed with intense resuscitation and massive transfusion initiated on placental circulation and after emergent cord clamping due to premature separation of the placenta, prior to complete resection of the mass.
CASE DESCRIPTION: A mother of a fetus, at 36 6/7 weeks gestation, with an estimated fetal weight of 2.5kg presented with a large anterior cervical neck mass with an intrathoracic extension involving compression of the trachea, right heart border and superior vena cava along with decreased fetal movement. Fetal ultrasound obtained showed scalp edema, ascites,and bilateral pleural effusions concerning for hydrops. Fetal echocardiography showed a dilated right ventricle, flattened intraventricular septum with qualitatively normal biventricular function. An emergent EXIT procedure was performed. Mass was found to be a highly vascular tumor which bled profusely during debulking, which included a sternotomy, prompting the initiation of intense resuscitation with intravenous and intracardiac epinephrine amounting to a total dose of 500 mcg, direct cardiac massage and massive transfusion while still on placental circulation and thereafter. A real time fetal echo was crucial in resuscitation. The fetal airway was secured by ENT under direct visualization emergently due to premature placental separation.Infant was transferred to an adjacent operating room for further tumor debulking. Blood loss was 1.5 liters. Our resuscitation required the administration of packed red cells, plasma, cryoprecipitate, platelets, bicarbonate and calcium gluconate approximating >600cc/kg over a period of 4 hours. The arterial blood gas at the end of the procedure: pH 7.28. PCO2 39,PO2 68,BE-7.8, Hb 8.9g/dl.
The infant was weaned off inotropic support in 48 hours and remained stable for a chest closure on the third postoperative day. MRI was negative for metastasis and pathology confirmed the diagnosis of infantile fibrosarcoma. The patient was able to be extubated to supplemental oxygen on day of life 16 and went home after 41 days in the neonatal ICU feeding well and gaining weight appropriately.
DISCUSSION: This is the first case reported in literature of this magnitude in intensity of resuscitation and massive transfusion during an EXIT procedure. The novelty and extreme nature of this case emphasizes the need for optimizing team work and planning, anticipation of potential emergent crises, and preparedness for intense resuscitation including massive transfusion during management of an EXIT procedure with a giant fetal neck mass.
-
 GA4-85 Image 1
GA4-85 Image 1
Top










