
OS2-143
Enhancing tonsillectomy patient care using outcomes-guided improvement cycles
Duling L, Allen T, Low D, Martin L
Seattle Childrens Hospital, Seattle, Washington, USA
Outcomes-guided improvement cycles were used to improve the anesthetic regimen for patients undergoing tonsillectomies and adenoidectomies (T&A) in a free-standing pediatric ambulatory surgery center. Best practice is typically adopted by ‘going to the literature’ for evidence-based practices and then replicating it. Despite T&A being a very common procedure performed in children, there is scant published evidence to inform best practice. Our group, agreed on a standardized anesthetic as a starting point then using Deming’s Plan-Do-Check-Act (PDCA) cycle of improvement; measured patient outcomes, and implemented iterative improvements.
Our goals were to create a standard anesthetic that (1) minimized or eliminated post-op pain and PONV while (2) not extending Post Anesthesia Care Unit (PACU) length of stay. Anesthesia was induced and maintained with sevoflurane, air, and oxygen. Propofol 1-2 mg/kg was used for airway instrumentation. Patients were given dexamethasone 0.15 mg/kg (max of 4 mg) and ondansetron 0.15 mg/kg (max 4 mg) and 20 ml/kg of lactated ringer. To eliminate variability in surgical technique, all procedures were performed by a single surgeon.
Three serial iterations of standard practice were tested in patients age 2-10y. Iteration 1 (C1): intraoperative (intraop) morphine 0.1 mg/kg (n= 439), iteration 2 (C2): intraop fentanyl 2.5 mcg/kg and acetaminophen 15 mg/kg (n= 273), and iteration 3 (C3): intraop morphine 0.1 mg/kg plus acetaminophen 15 mg/kg (n= 266). The primary outcome was maximum post-op pain score. Secondary outcomes measured were morphine rescue rate in PACU, PACU length of stay, and PONV rescue rate. Each cycle was instituted and measured for a period of 11-18 months.
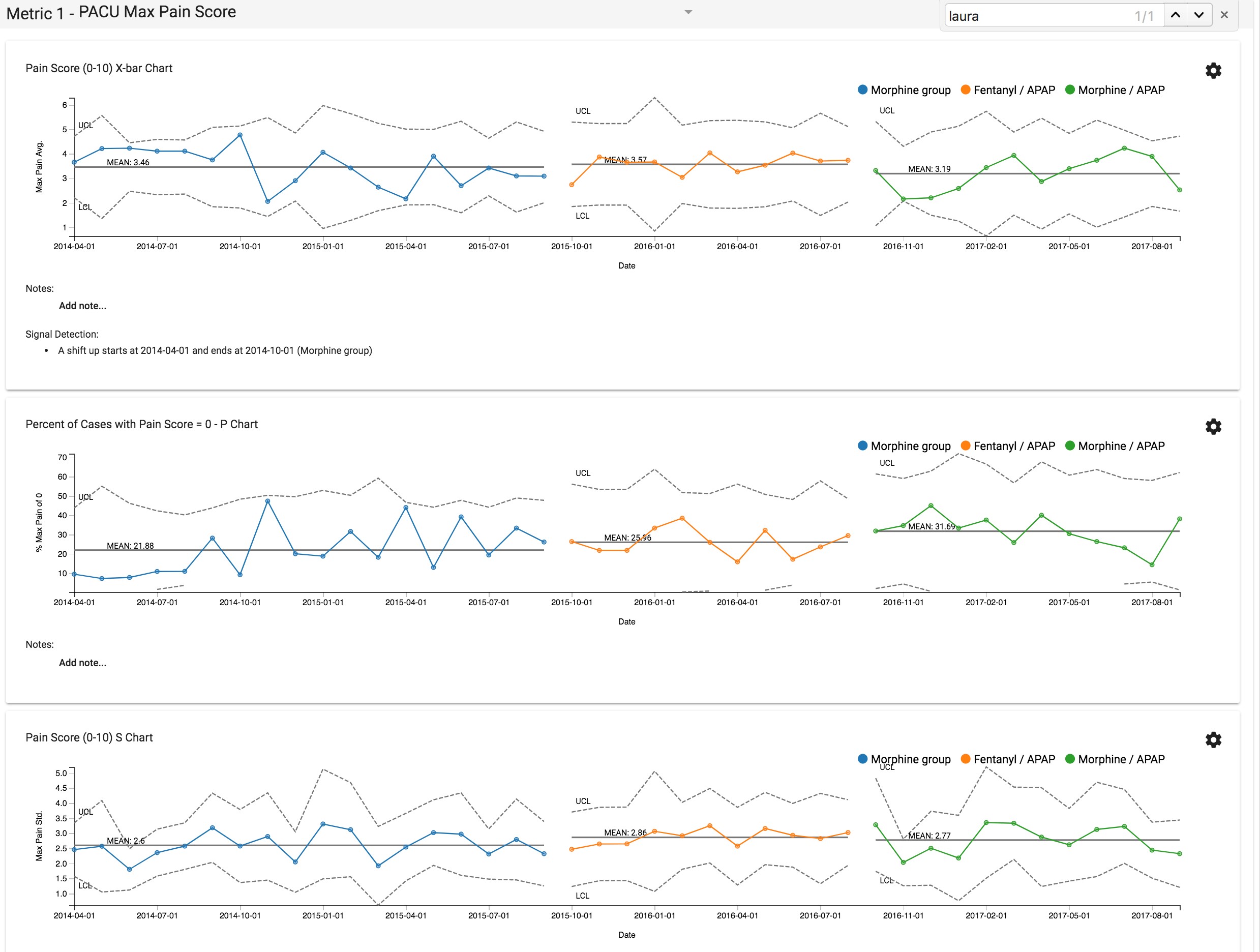
The above outcomes were retrospectively compared using QI Advisor (www.mdmetrix.com) which interrogates the clinical database to give near-real time analysis. Shewhart charts were created to demonstrate stable outcomes and to look for special cause variation.
Average max pain score for PACU stay: C1 = 3.46, C2= 3.57, C3 = 3.19; with C3 (morphine and acetaminophen) having lowest max pain score (Chart 1). The percent of patients that achieved a zero pain score during the PACU stay: C1 = 20.8%, C2 = 25.9%, C3 = 30.5%, with C3 providing the most pain free PACU stay. Morphine rescue: C1 =13%, C2 = 15.9%, C3 = 14.9%. PONV reported, defined as needing additional PONV medication: C1 = 4.6%, C2 = 1.9%, C3 = 0.4%; again, C3 had the lowest rate of additional PONV medications. Length of stay was unchanged for all groups (71min, including awake PACU extubation).
These data suggest that a morphine and acetaminophen combination provide the lowest pain scores while maintaining a low requirement for rescue PONV medication without lengthening PACU stay. Using these outcomes-guided improvement cycles of clinical standard work for T&A surgery has allowed our group to safely evolve our anesthetic practice to improve care for our patients.
-
 OS2-143 Image 1
OS2-143 Image 1
Top










