
GA4-88
Development and utilization of a standardized postoperative clinical care pathway for reduction in hospital length of stay following minimally invasive repair of pectus excavatum
1Mecoli M, 1Tuncel-Kara S, 1Rogers T, 1Platt M, 1Chidambaran V, 2Sadhasivam S, 1Brown R, 1Garcia V
1Cincinnati Children's Hospital Medical Center, Cincinnati, OH, USA; 2Riley Hospital for Children, Indianapolis, IN, USA
Introduction: Recent trends in healthcare payment models encourage healthcare providers to increase coordination of care, improve quality, and reduce cost (1). Application of standardized postoperative clinical care has been shown to reduce hospital length of stay (LOS) in major orthopedic surgery (2). The aim of this study was to develop and implement a standardized clinical care pathway (SCCP) for patients undergoing minimally invasive repair of pectus excavatum (MIRPE). We hypothesized that strict adherence to a SCCP would result in decreased LOS without negatively affecting post-discharge metrics.
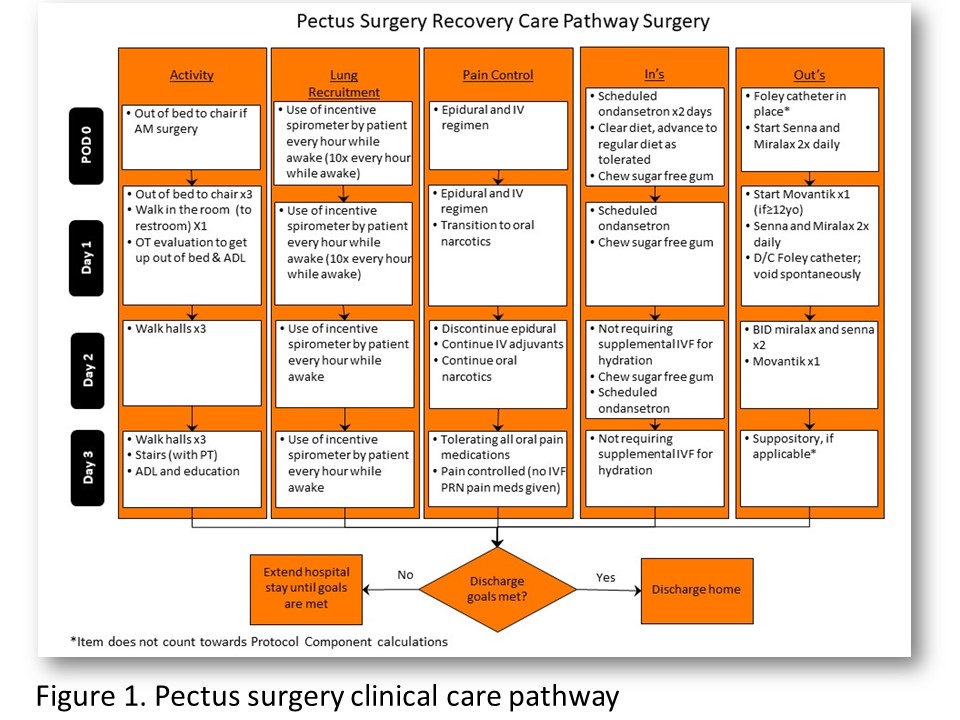
Methods: An interdisciplinary team of surgeons, pain specialists, advanced nurse practitioners, and quality improvement specialists developed a SCCP specific to pectus surgery and included 42 measurements under 5 main components: mobility, lung recruitment, daily oral intake and output, and pain management (FIG 1). Primary outcome was LOS measured in postoperative nights and secondary outcomes included post-discharge pain, mobility, and hospital readmission. Pain management protocol was modified for the pathway and included the use of non-narcotic adjuvants, epidural analgesia with discontinuation of epidural on POD 2, and expectation for pain to be primarily managed with oral medications on POD 3. We tracked pathway compliance through chart review, and telephone surveys were performed following discharge.
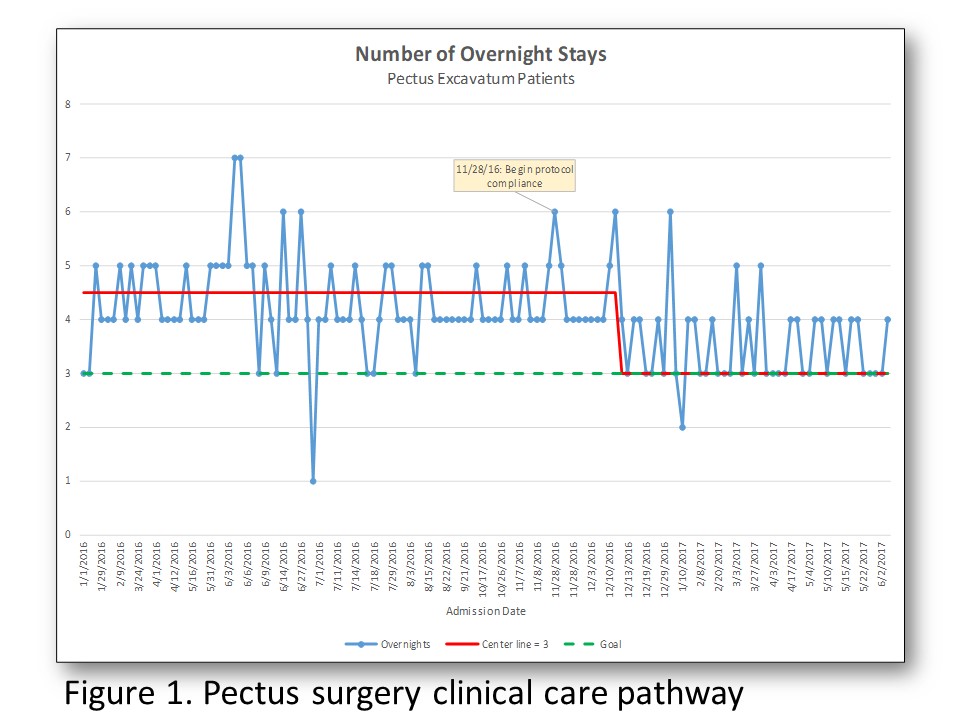
Results: The total patients included were n=134 (n=78 pre-protocol and n=56 post-protocol) between 1/2016 and 6/2017. Baseline compliance with protocol elements was 74%; compliance was increased to 96% within one month after protocol implementation and was sustained throughout the study period. There was a reduction in LOS from a median 4.5 days to 3 days following protocol implementation (FIG 2). 51 patients were called following discharge and 27 phone surveys were completed (response rate 53%). 80% of patients reported NRS pain score 4 or less and 70% reported mobility level of 7 or more (0=not mobile and 10=independent). There was no change in hospital readmission with 2.5% (n=2) before and 3.5% (n=2) after implementing the protocol.
Conclusions: A multidisciplinary standardized postoperative care pathway with multimodal analgesia was implemented for patients following MIRPE. Strict adherence to the pathway was achievable and resulted in reduced time to functional recovery as reflected by shorter LOS. Most patients reported good pain control and mobility following discharge and there was no increase in hospital readmissions.
References:
1.Sood, N et al. Health Aff (Millwood) 2011; 30(9): 1708-1717
2.Muhly, W et al. Pediatrics 2016;137
-
 GA4-88 Image 2
GA4-88 Image 2 -
 GA4-88 Image 1
GA4-88 Image 1
Top










