
CR1-180
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) in the apnic child: a mini-case series
Carver M, Carver M
CHLA, Los Angeles, CA, United states
Intro:
Recently there has been an increasing interest in the use of supplemental oxygen during airway management. Oxygen delivery throughout the entire process of intubation results in longer durations before desaturation for both spontaneously breathing and apneic patients (apneic oxygenation). Pediatric data regarding supplemental oxygen during airway management is unfortunately lagging behind, despite the fact that children desaturate quicker than adults.
One modality that is gaining appeal is the use of High Flow Nasal Cannula (HFNC) also known as Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) which has already shown considerable benefit in pediatric critical care patients with respiratory distress. Anesthesiologists are starting to look at this method in both adults and kids for airway management. The key advantage of HFNC over traditional oxygen delivery is not only improved oxygenation but also the creation of positive pressure via rapid flow rates (up to 2 L/kg/min), and due to a vortex induced diffusion gradient, it can provide apneic ventilation / CO2 exchange1. This slows hypercarbia and respiratory acidosis during apneas. To date, there is only one study looking at THRIVE in pediatric airway management, which showed prolonged apneas without desaturations2.
Case:
Our goal in studying THRIVE in the OR setting is to determine its benefit and use in airway procedures that often require complex coordination with surgeons. We hypothesize that by utilizing HFNC, patients even if apneic, will have prolonged times before desaturation and delayed hypercarbia.
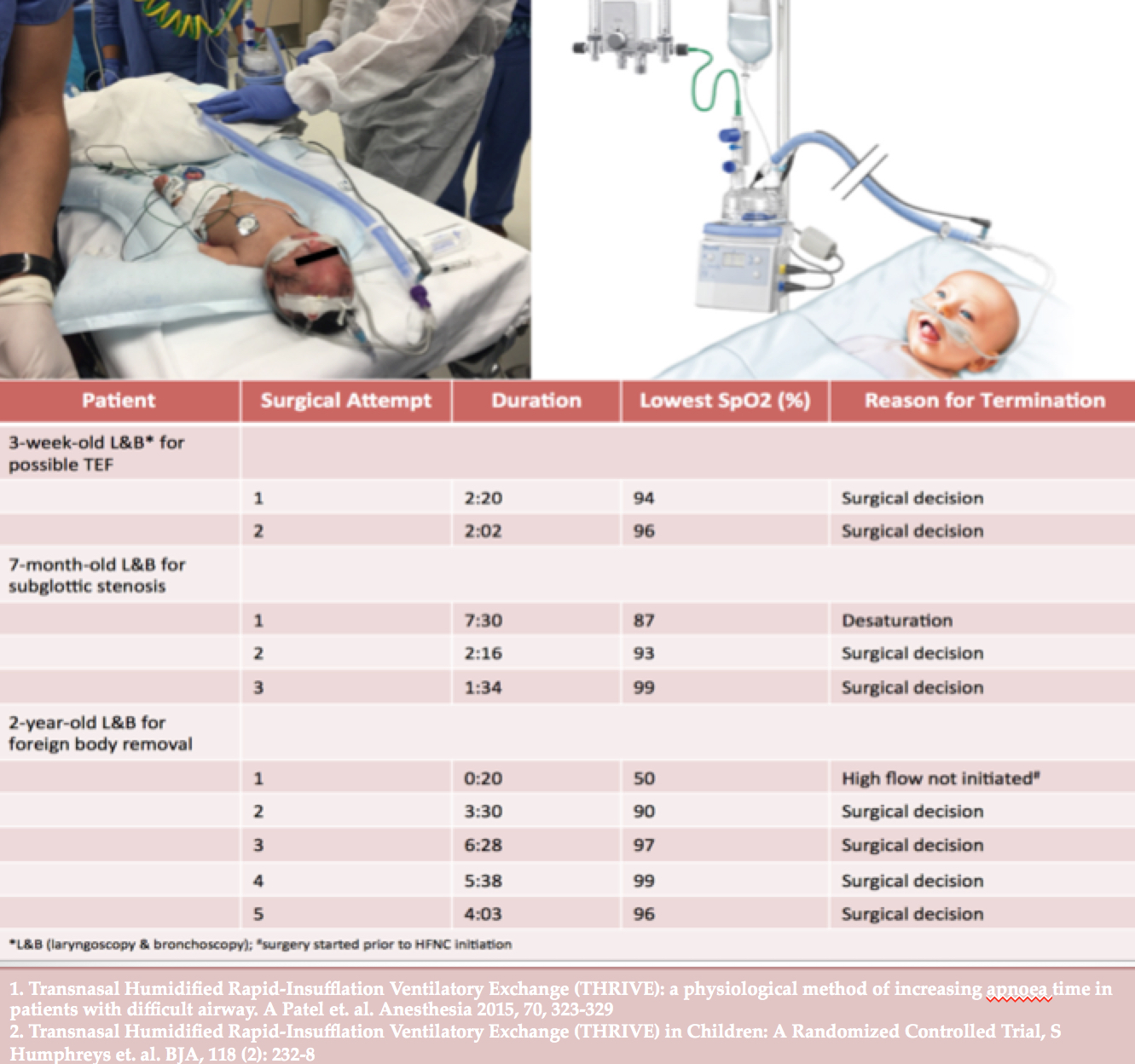
Complex airway surgeries often result in multiple airway instrumentations, desaturations, interruptions, hypercarbia etc. We present 3 patients who while undergoing ENT surgery were placed on HFNC. In all three, apnea was encountered for differing reasons including anesthetic sensitivity, surgical compression or blockage of the airway.
Our preliminary results are encouraging- each patient lasted well beyond what would be expected before desaturation especially given their age. In all but one case, oxygen saturation remained in the 90’s and apnea was only stopped for either surgical completion or to mask-ventilate between surgical stages. All patients remained thermodynamically stable
Discussion:
HFNC has an established benefit in the PICU and provides oxygenation, ventilation support and decreased work of breathing in critically ill children. As we begin to better understand the benefits HFNC offers to the anesthesiologist, we can apply this technique to the OR for both difficult airway management & airway surgeries. Our results although preliminary, are the first findings to support using THRIVE to decrease hypoxemia during apneic events. It also provides surgeons with less interrupted surgical conditions potentially allowing for expedited procedures, decreased operative time and hopefully with enough power- will show reduced adverse events
-
 CR1-180 Image 1
CR1-180 Image 1
Top










