
GA1-44
Optimization of COLDS scoring system: A pre-anesthetic risk assessment tool
Shaw R, Bernardo M, Ren W, Lee L
UCLA, Los Angeles, CA, USA
Background: Upper respiratory tract infections (URIs) in the pediatric population are frequently encountered in the perioperative setting. Anesthesia providers need to utilize various tools in order to deem a patient safe to proceed with surgery. The COLDS score was developed by Lee and August as a way to risk stratify pediatric patients with upper respiratory infections. Previously we showed that this score has a good predictive value for perioperative respiratory complication (AUC=0.69), however we postulated that there was room to improve this scoring system. This study aimed to optimize the current COLDS score to yield better predictive value.
Methods: IRB approval was obtained prior to data collection. Patients 6 years old and under presenting for any type of procedure were included. Exclusion criteria were current endotracheal tube or tracheostomy and patients with congenital heart disease. For optimization of the COLDS score, we attempted to improve the predictive ability of the scoring system by changing the key from a 1, 2 and 5 score for each category to one determined by integerizing the beta values obtained by logistic regression. We also attempted to improve the predictive ability of COLDS by weighting each of the 5 categories that compose the COLDS Score by logistic regression. Finally, we created a Cox proportional hazards model to predict the likelihood of any perioperative respiratory complication and a negative binomial model to predict the number of expected perioperative respiratory complications with a given COLDS score.
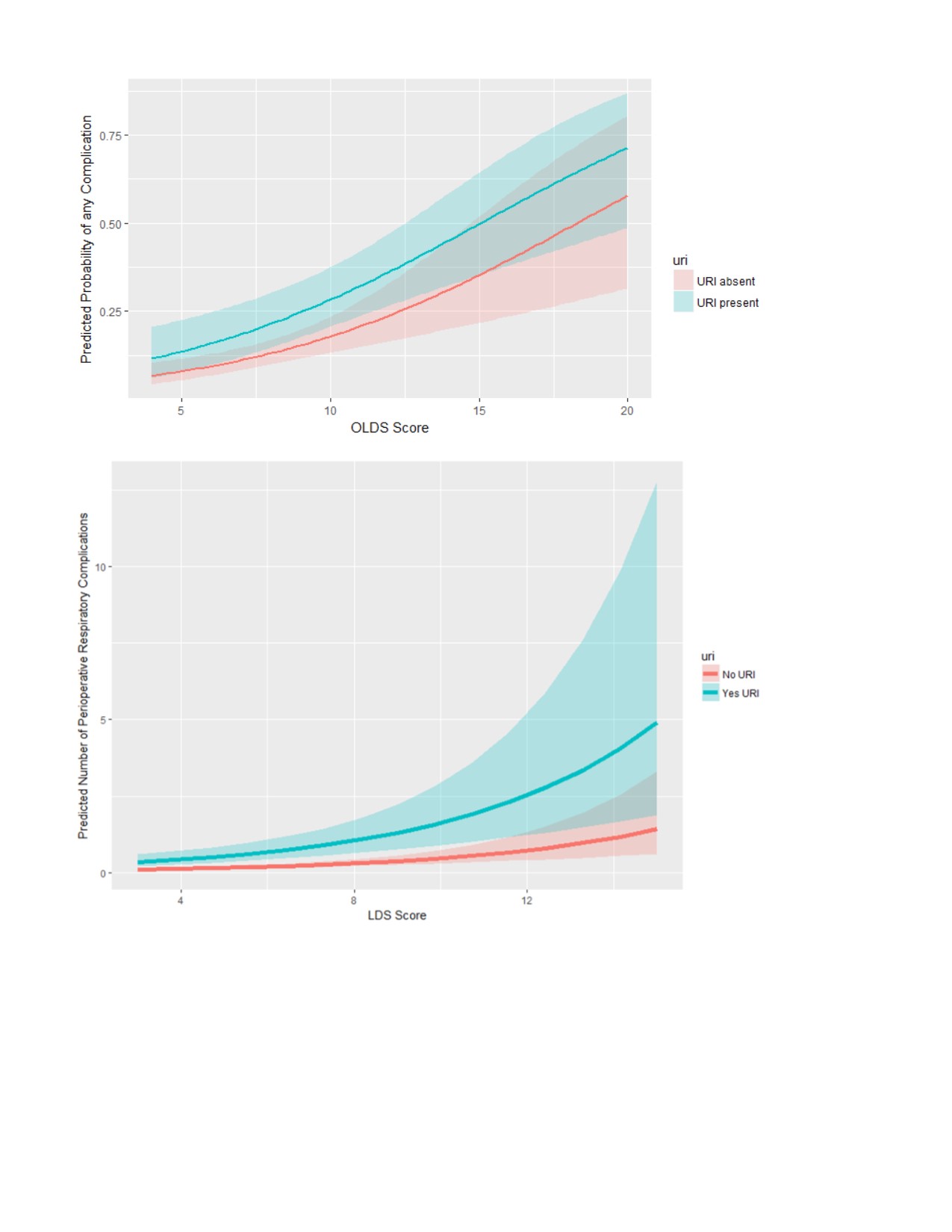
Results: Data was collected on 436 patients over 6 months. Re-keying of the COLDS score improved AUC to 0.70, while reweighting the COLDS score categories improved the AUC to 0.71. We found in our logistic regression model that the terms for onset and surgery type were not significant. Removing these from the COLDS score (CLD score) yielded an AUC of 0.70. Since the real question to be answered is whether to proceed or not with a recent URI, rather than whether or not to have the surgery at all, we separated the variable risk factor of having a URI, from the rest of the immutable risk factors (lung disease, airway device to be used and surgery type) and created a Cox Proportional Hazards model and a negative binomial model to show risk of perioperative respiratory complications with and without URI.
Discussion/Conclusions: The re-keying of the COLDS score greatly increased the complexity of the scoring system without commensurately improving its predictive value, so the 1, 2, 5 scoring key is good as it stands. Reweighting the categories did improve its predictive value. The predictive models presented may be useful as teaching tools for providers to their families about the expected increase in risk of a respiratory complication when the patient has had a recent URI. Additionally, this validated scoring system can be a useful decision-making tool for practitioners.
-
 GA1-44 Image 1
GA1-44 Image 1
Top










