
AIR-13
Prone Intubation through an Air-Q in a Difficult to Ventilate and Intubate Neonate with Desbuquois Dysplasia
Jensen B, Le S, Lo C
Children's Hospital Los Angeles, Los Angeles, CA, USA
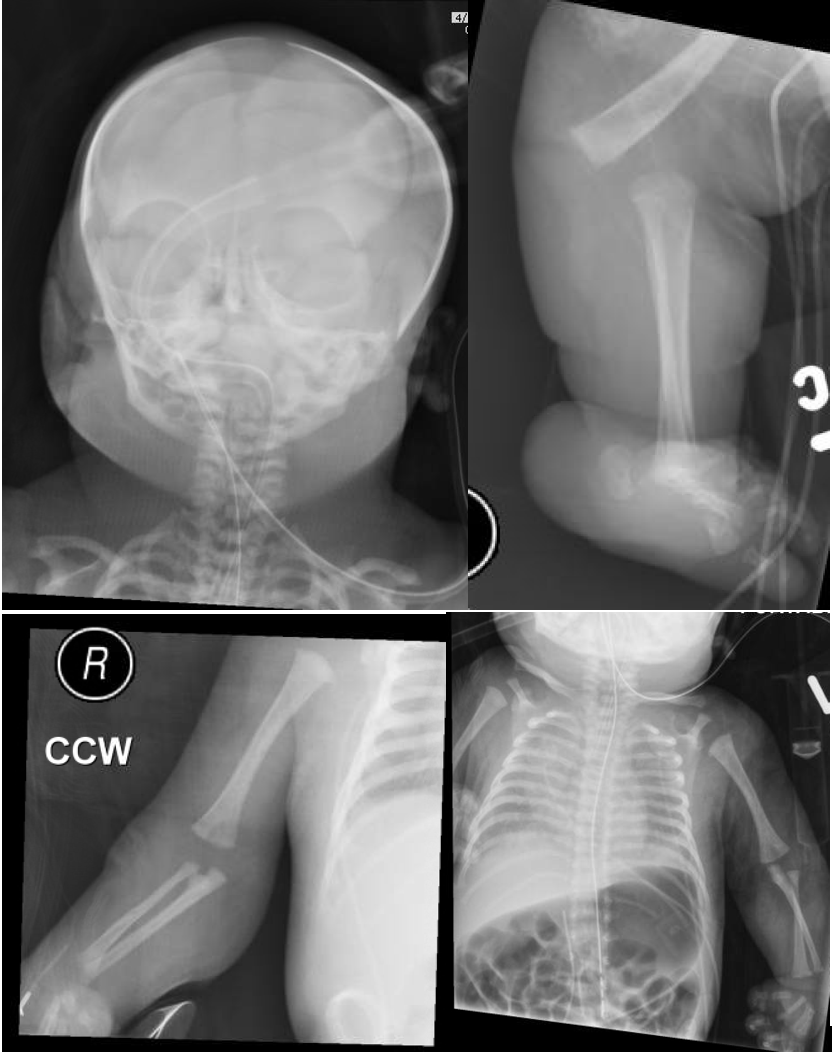
Introduction: Less than 50 cases of Desbuquois Dysplasia have been described in literature.2 Previously published literature described successful ventilation in a patient with Desbuquois Dysplasia using a Cobra perilaryngeal airway.1 However, endotracheal intubation through this device was not possible. Our case describes a pediatric patient with this syndrome that was successfully intubated with a fiberoptic scope via an Air-Q LMA in the prone position.
Case Presentation: A 3-day old, 2.1 kg full term baby girl with prenatal diagnosis of cleft palate, retrognathia, and other abnormalities was transferred to our hospital for management of respiratory distress. A genetics workup would later reveal that the patient had a diagnosis of Desbuquois Dysplasia. On admission, the patient only tolerated the prone position with a nasal cannula, and would desaturate in the supine position.
Anesthesia was called for urgent intubation given the worsening respiratory status. The patient was transported to the operating room with standard ASA monitors in the prone position on nasal cannula. In the OR, Glycopyrolate (0.1 mg), Dexmedetomidine (0.5 mcg/kg), and Ketamine (2 mg/kg) were slowly titrated in with maintenance of spontaneous ventilation. Our attempt to bag-mask ventilate the patient in the supine position with an oral airway and two-handed technique was unsuccessful. Oxygen saturation improved when the patient was masked in the prone position with her head turned to the side. A 0.5 Air-Q LMA was inserted in the prone position with subsequent easy ventilation. To secure the airway, a 2.8 mm fiberoptic bronchoscope was passed through the swivel adaptor/Air-Q with a 3.0 uncuffed endotracheal tube (ETT) loaded. After confirmation of ETT placement with the fiberoptic scope and capnography, the patient was paralyzed with Rocuronium (1 mg/kg). The patient was transported to the NICU in a stable condition. A tracheostomy was placed at a later date, and the patient was placed on hospice care two months later.
Discussion: Our case described a successful prone intubation in a 2.1 kg neonate with Desbuquois Dysplasia. The unique aspect of this intubating scenario was the inability of the patient to tolerate the supine position. Therefore, common airway techniques by ENT surgeons such as rigid bronchoscopy and tracheostomy would not be feasible. We demonstrated the first successful example of a prone intubation through an Air-Q LMA using a fiberoptic scope in this difficult patient population. Our technique may be applied to other syndromic patients that only tolerate prone positioning.
References:
1. SZMUK, PETER, et al. “Use of CobraPLATM for Airway Management in a Neonate with Desbuquois Syndrome. Case Report and Anesthetic Implications.â€Â Ped Anes, Blackwell Science Ltd, 14 June 2005.
2. “The Portal for Rare Diseases and Orphan Drugs.†Orphanet: Desbuquois Syndrome, www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=GB&Expert=1425
-
 AIR-13 Image 1
AIR-13 Image 1
Top










