
NM-378
Fibrinogen Concentrate Versus Cryoprecipitate in Restoring Hemostasis in Infants After Cardiopulmonary Bypass
1Downey L, 1Lilien M, 1Austin T, 1Guzzetta N, 2Miller K
1Emory /Children's Healthcare of Atlanta, Atlanta, GA, United states; 2Children's Healthcare of Atlanta, Atlanta, GA, United states
Introduction
After cardiac surgery with cardiopulmonary bypass (CPB), infants often develop acute acquired hypofibrinogenemia that contributes to impaired fibrin formation and inadequate clot formation. Cryoprecipitate is currently the standard of care to supplement fibrinogen. However, fibrinogen concentrate (FC) (Riastap®, CSL Behring, Kankakee, IL), an FDA approved form of purified fibrinogen, has several advantages over cryoprecipitate: 1) smaller volume; 2) accurate dosing; 3) immediate availability; 4) lower risk of infectious transmission; 5) lower risk of allergic and immunologic reactions. In this study, we compared the use of FC to cryoprecipitate as part of our post-bypass transfusion algorithm in infants after cardiac surgery.
Methods
After IRB approval and parental consent, we prospectively randomized infants (greater than 32 weeks gestational age and with no personal or family history of thrombosis) to receive either 2 units of cryoprecipitate or FC. We targeted a post-transfusion fibrinogen level of 300 mg/dL as part of our post-bypass hemostasis algorithm. Claus fibrinogen levels, thromboelastograms (TEG) and TEG functional fibrinogen (TEG-FF) were drawn at four time points: before CPB (baseline), on CPB, post-transfusion, and on arrival to the ICU. We compared fibrinogen levels and TEG-FF parameters (MA-FF and FLEV) between the two groups.
Results
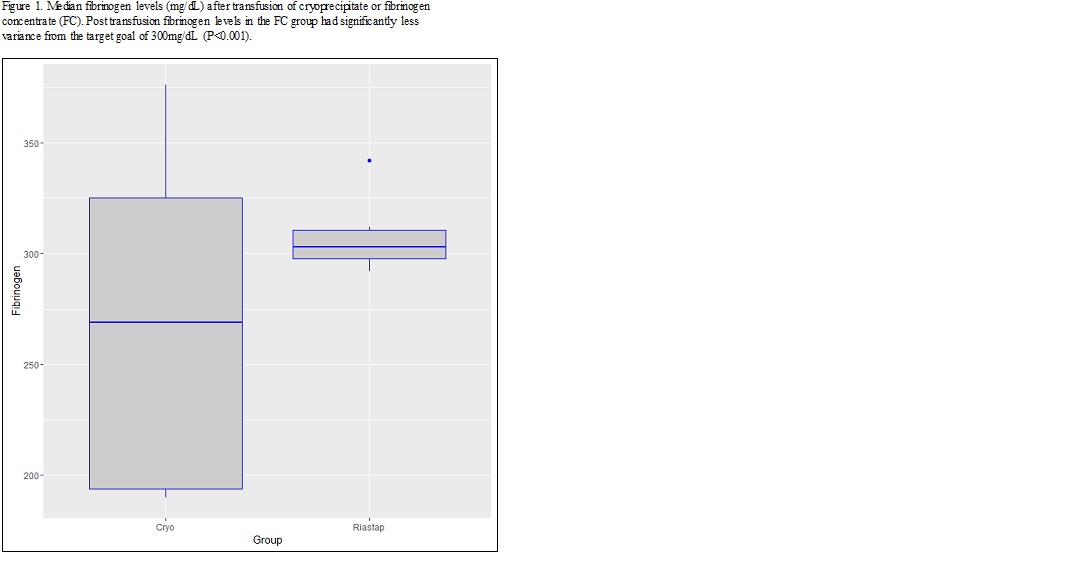
Nine patients received cryoprecipitate (mean age 5.4 months + 1.7; range: 1-10 months) and nine received FC (mean age 4.0 months + 2.7; range: 0-9 months). There was no significant difference between the two groups in fibrinogen, FLEV, or MA-FF values immediately post-transfusion or in the ICU. However, the FC group more precisely achieved the targeted fibrinogen level (300 mg/dL), with significantly less variability compared to the cryoprecipitate group (p <0.001) (Figure 1). Pre-CPB fibrinogen values did not correlate with FLEV in either arm. However, after transfusion of adult fibrinogen, both the cryoprecipitate and FC groups demonstrated correlation between Claus fibrinogen and FLEV values (R = 0.769, p = 0.015; R = 0.762, p = 0.017 respectively).
Discussion
Given the safety concerns associated with blood product administration, we compared FC to cryoprecipitate as part of our post-bypass transfusion algorithm in achieving a targeted fibrinogen level and clot strength using TEG-FF. Administration of FC achieved a targeted fibrinogen level more precisely than cryoprecipitate. Patients in both groups achieved similar MA-FF and FLEV values, suggesting no difference in functional fibrinogen between sources of fibrinogen. In conclusion, FC is an effective alternative to cryoprecipitate for achieving adequate fibrinogen levels and clot strength in infants undergoing cardiac surgery with CPB.
-
 NM-378 Image 1
NM-378 Image 1
Top










