
OS2-151
Predictors of Transfusion Outcomes in Pediatric Complex Cranial Vault Reconstruction
1Fernandez P, 2Taicher B, 3Gangadharan M, 4Goobie S, 5Stricker P, 1Skitt R, 2Homi H, 6Kugler J
1Children's Hospital Colorado, Aurora, CO, USA; 2Duke University Medical Center, Durham, NC, USA; 3University of Texas Medical Branch, Galveston, TX, USA; 4Boston Children's Hospital, Boston, MA, USA; 5The Children's Hospital of Philadelphia, Philadelphia, PA, USA; 6Children's Hospital & Medical Center, Omaha, NE, USA
INTRODUCTION
Pediatric patients undergoing complex cranial vault reconstruction (CCVR) are at risk for significant blood loss requiring perioperative transfusion. Minimizing blood loss and transfusion are important goals due to the risks and cost of allogenic blood transfusion. Various strategies are often employed to minimize blood product exposure; however, the impact of patient and surgical variables on transfusion is unknown. We evaluated independent associations of demographic and perioperative variables with transfusion outcomes in CCVR.
METHODS
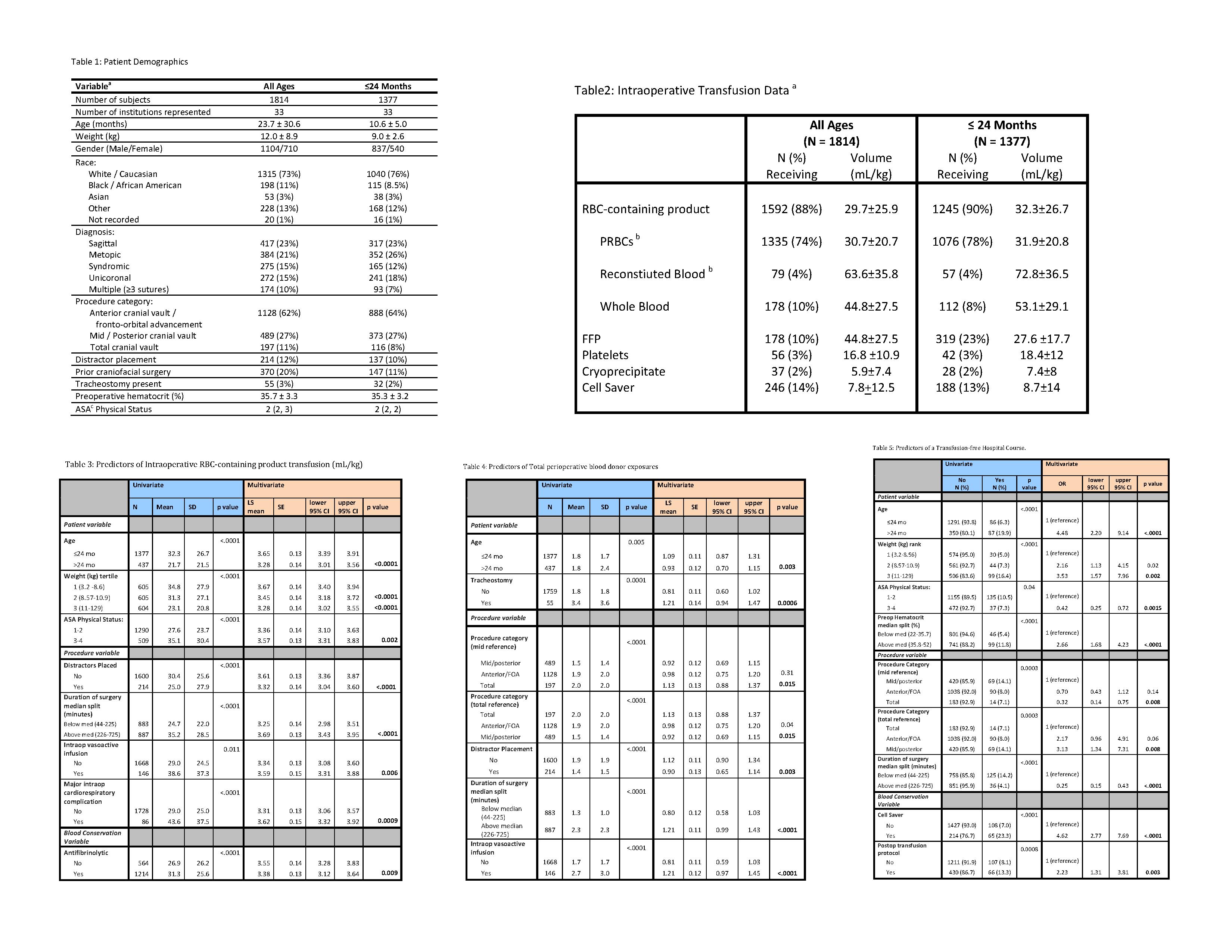
Query for CCVR in the pediatric craniofacial surgery perioperative registry resulted in demographic and perioperative data from 33 institutions encompassing 5-years. Three transfusion outcomes were analyzed: intraoperative red blood cell-containing product (IRBC-CP) transfusion, total perioperative blood donor exposures (BDE), and a transfusion-free hospitalization (TFH). Univariate and multivariate analyses were performed for variables related to patient, procedure and blood conservation techniques potentially associated with these three outcomes.
RESULTS
1,814 cases were analyzed: 75% were <24 months old and 90% received IRBC-CP. Among significant predictors of IRBC-CP transfusion were age, ASA physical status, surgical duration, and antifibrinolytic administration. Age, tracheostomy presence, distractor placement, surgical duration and total cranial vault reconstruction were independently associated with increased BDE. Age > 24 months (OR 4.5), weight > 11kg (OR 3.5) and preoperative hematocrit >35.8 (OR 2.7) were more likely to experience TFH; while those with ASA physical status > 3 or a surgical duration > 225 minutes were less likely. Blood conservation techniques predictive of TFH included use of cell saver (OR 4.6) and use of a postoperative transfusion protocol (OR 2.2).
DISCUSSION
Minimizing blood loss and transfusion is important due to the risks and cost of allogenic blood transfusion. While demographic variables such as age, weight and ASA status are relatively fixed, we report 4 modifiable factors that could decrease allogenic blood transfusion in CCVR. Ensuring a higher preoperative hematocrit, utilizing cell saver, using antifibrinolytics and introducing postoperative transfusion protocols are all modifiable factors that may be impactful. Future study of transfusion outcomes in CCVR should include these goals.
CONCLUSION
Interventions likely to have an impact on transfusion outcomes in pediatric CCVR include a goal pre-operative hematocrit > 35.8, use of intraoperative cell saver, utilizing antifibrinolytics and the institution of a postoperative transfusion protocol.
REFERENCE:
1. Stricker PA et al. Perioperative Outcomes and Management in Pediatric Complex Cranial Vault Reconstruction: A Multicenter Study from the Pediatric Craniofacial Collaborative Group. Anesthesiology. 2017; 126: 276-287
-
 OS2-151 Image 1
OS2-151 Image 1
Top










