
AET-30
Intraoperative Point-of-Care Ultrasound for Identification of Endotracheal Tube Position in the Pediatric Population
Goltiao D, Ghazal E, Ramsingh D, Pugh J, Ross P
Loma Linda University, Loma Linda, CA, USA
Introduction
Anesthesiologists rely on auscultation and clinical exam to determine correct endotracheal tube (ETT) placement since CXR or fluoroscopy are rarely available. Studies have shown that 18-19% of all intubations result in inappropriate ETT placement and up to 11% of malpositioned ETT are not recognized.{1,2} Recently, utility of point of care ultrasound (POCUS) to identify appropriate placement of the ETT in adults has been demonstrated.{3} However, similar utility has yet to be determined in pediatrics. This study aims to evaluate the utility of a POCUS exam to identify appropriate ETT position in a pediatric population by examining measurements of the ultrasound (US) examination to those from routine fluoroscopy.
Methods
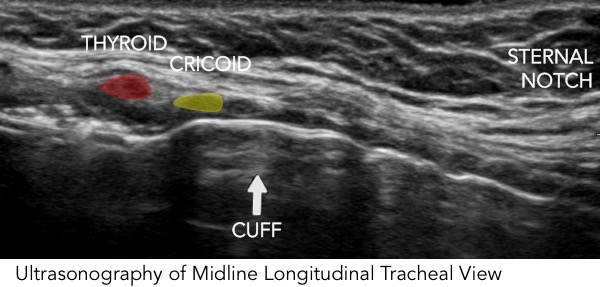
Pediatrics (<10 years) requiring cuffed ETT for cardiac cath procedures involving chest fluoroscopy were consented. Patients underwent induction and standard verification of ETT positioning. Then, with an US linear probe placed in a midline longitudinal tracheal view, ETT cuff was identified by assessing for tracheal motion during palpation of the pilot balloon. Measurements of cuff relative to sternal notch, cricoid cartilage, and thyroid cartilage were obtained. Transverse tracheal view was visualized to identify the location of the esophagus and bilateral pleural lung sliding was also evaluated. Chest fluoroscopy was reviewed to assess ETT in relationship to the carina. Primary comparison was correlation assessment between the US measurements to the fluoroscopy measurements. In addition, incidence of inappropriate ETT location was compared between the auscultation and both the US and fluoroscopy examinations. Time to perform the POCUS exam was recorded.
Results
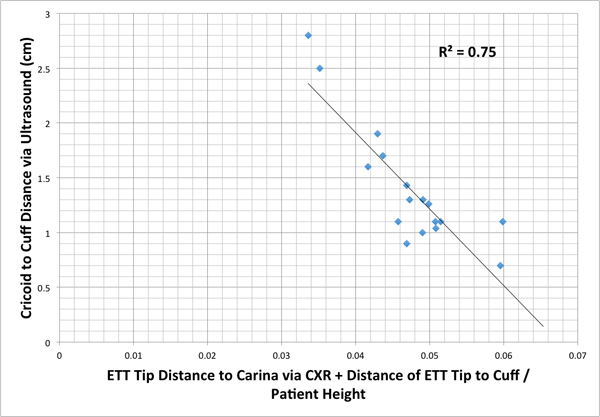
Preliminary results (n= 32) indicate 100% detection/visualization of the ETT cuff with the POCUS exam. Average time to perform the exam was 163 secs (stdev = 67sec). A strong correlation (R=-0.87) was demonstrated between the US measurements to the fluoroscopy measurements (p <.001). (Figure 1) Additionally, the POCUS exams have demonstrated 100% visualization of the esophagus, with 66% demonstrating the esophagus to be to the left of the trachea.
Conclusion
Preliminary data suggests that airway POCUS is a fast and reliable modality to verify adequate depth of the ETT in the pediatric population.
References
Harris, E. Endotracheal Tube Malposition within the Ped Population. Can J Anesth(2008)
Verghese, S. Auscultation of Bilateral Breath Sounds Does not rule out Endobronchial Intubation in Children. Anesth & Analgesia(2004)
Ramsingh, D. Auscultation vs Point-of-care Ultrasound to Determine Endotracheal vs Bronchial Intubation. Anesth(2016)
-
 AET-30 Image 2
AET-30 Image 2 -
 AET-30 Image 1
AET-30 Image 1
Top










