
CA-41
Muscle Oxygenation in Children with Congenital Heart Disease
1Ross F, 2Arakaki L, 2Ciesielski W, 1McMullan D, 1Richards M, 1Geiduschek J, 1Latham G, 1Hsieh V, 1Joffe D, 2Schenkman K
1Seattle Children's Hospital, Seattle, WA, United states; 2University of Washington, Seattle, WA, United states
Introduction
Children with congenital heart disease (CHD) undergo adaptive responses to chronic cyanosis to maintain adequate tissue oxygenation. (Adatia 1993, PMID 8149686) It is unknown whether such adaptation maintains normal oxygen (O2) metabolism in peripheral muscle. We developed a noninvasive monitor that determines muscle oxygenation (MOx) by measuring differences between oxygenated and deoxygenated hemoglobin and myoglobin. (Arakaki 2013 PMID, 23764440) Since MOx accounts for the oxygen bound to both hemoglobin and myoglobin, it reflects the total O2 available within the muscle tissue. During an abrupt interruption of the O2 supply by arterial occlusion, the change in MOx measured during the first minute is directly related to the pre-occlusion steady-state O2 consumption. (Gurley 2012, PMID 22894483) This study aimed to determine the difference in resting muscle oxygenation and the rate of O2 consumption in children with cyanotic and acyanotic CHD. This knowledge will help determine if MOx may serve as a sensitive monitor to guide hemodynamic management of these patients.
Methods
Optical spectra were acquired with a system consisting of a custom fiber optic probe, an LED light source, and an imaging spectrometer. Measurements were obtained from the calf or forearm of 49 patients (17 acyanotic CHD, 18 cyanotic CHD, and 14 control). 20 additional control patients were used to develop the analytic model. For CHD patients, measurements were taken at baseline on 100% O2, during 3-min arterial tourniquet occlusion, and during reperfusion. For control patients, the arterial occlusion was 15 min long to obtain complete desaturation for model development and testing. Each CHD group was compared to controls using two-sample t-tests. Significance was defined as p<0.05.
Results
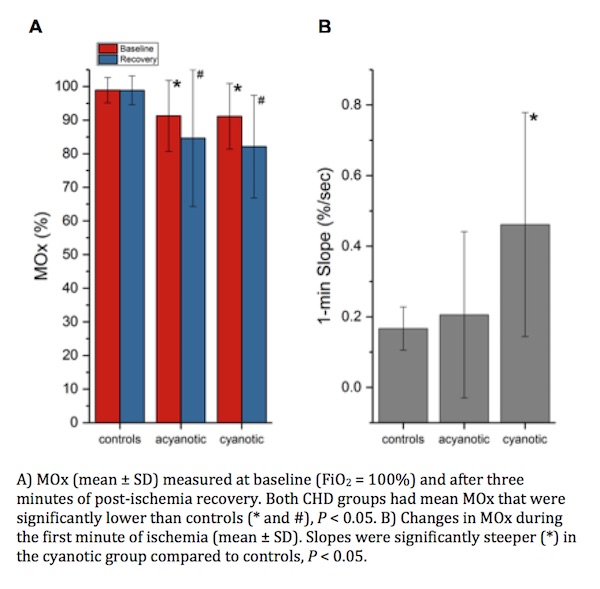
Patients with acyanotic and cyanotic CHD had lower baseline MOx than controls (Fig. A, red bars). Similarly, MOx was lower in the acyanotic and cyanotic groups than controls after reperfusion, despite shorter arterial occlusion in these groups (Fig. A, blue bars). The rate of decline in oxygenation (slope ΔMOx/t) was greater in cyanotic patients vs. controls (Fig. B) but similar between acyanotic patients and controls.
Discussion
Both cyanotic and acyanotic patients had low MOx, indicating limited oxygen supply at baseline. In acyanotic patients, low cardiac output and decreased blood flow to peripheral muscles are plausible explanations for low baseline MOx. Acyanotic patients had 1-min slopes comparable to controls, suggesting normal oxygen consumption. Cyanotic patients had more rapid O2 decline, suggesting either increased metabolic rate or more likely, limited intracellular O2 reserves. Thus, these patients are particularly vulnerable to ischemic insults.
Conclusions
This study demonstrates that MOx is abnormal in cyanotic and acyanotic CHD patients. Thus, monitoring MOx perioperatively may provide valuable information in this population.
-
 CA-41 Image 1
CA-41 Image 1
Top










