
NM-221
Intraoperative Ketorolac after Achieving Hemostasis in Pediatric Tonsillectomy Improves Perioperative Analgesia Outcomes without Increasing Post-tonsillectomy Bleeding
1Ence B, 2Rabbani C, 2Pflum Z, 2Ye M, 2Gettelfinger J, 2Matt B, 2Dahl J, 1Sadhasivam S
1Riley Hospital for Children at Indiana University Health, Indianapolis, IN, USA; 2Indiana University School of Medicine, Indianapolis, IN, USA
Introduction: Ketorolac is a non-steroidal anti-inflammatory drug that has been shown to be effective at reducing postoperative pain without the risk of sedation, vomiting, and respiratory depression common with opioids. However, use of intraoperative ketorolac for tonsillectomy is controversial due to possible increased risk of post-tonsillectomy bleeding. Consensus is lacking on the risk of post-tonsillectomy hemorrhage, as well as optimal timing of intraoperative ketorolac to minimize bleeding risks and improve postoperative analgesia. The aim of this retrospective study is to contribute to an understanding of the safety and efficacy of administering ketorolac intra-operatively after achieving hemostasis following tonsillectomy in children.
Methods: After obtaining IRB approval, children undergoing tonsillectomy, aged 4 -18 years, between 2013 and 2017 were included in this retrospective study. Otolaryngologists, based on hemostasis following tonsillectomy, requested the anesthesia team to administer or not to administer intravenous ketorolac (0.5 mg/kg) intra-operatively. Peri-operative records, including intra-operative anesthesia and post-anesthetic care unit (PACU) records were reviewed. Demographic characteristics, medical history, post-operative hemorrhage, medication administration, and oral intake were reviewed. Post-tonsillectomy hemorrhage, inpatient oral intake, analgesia and opioid administration were examined.
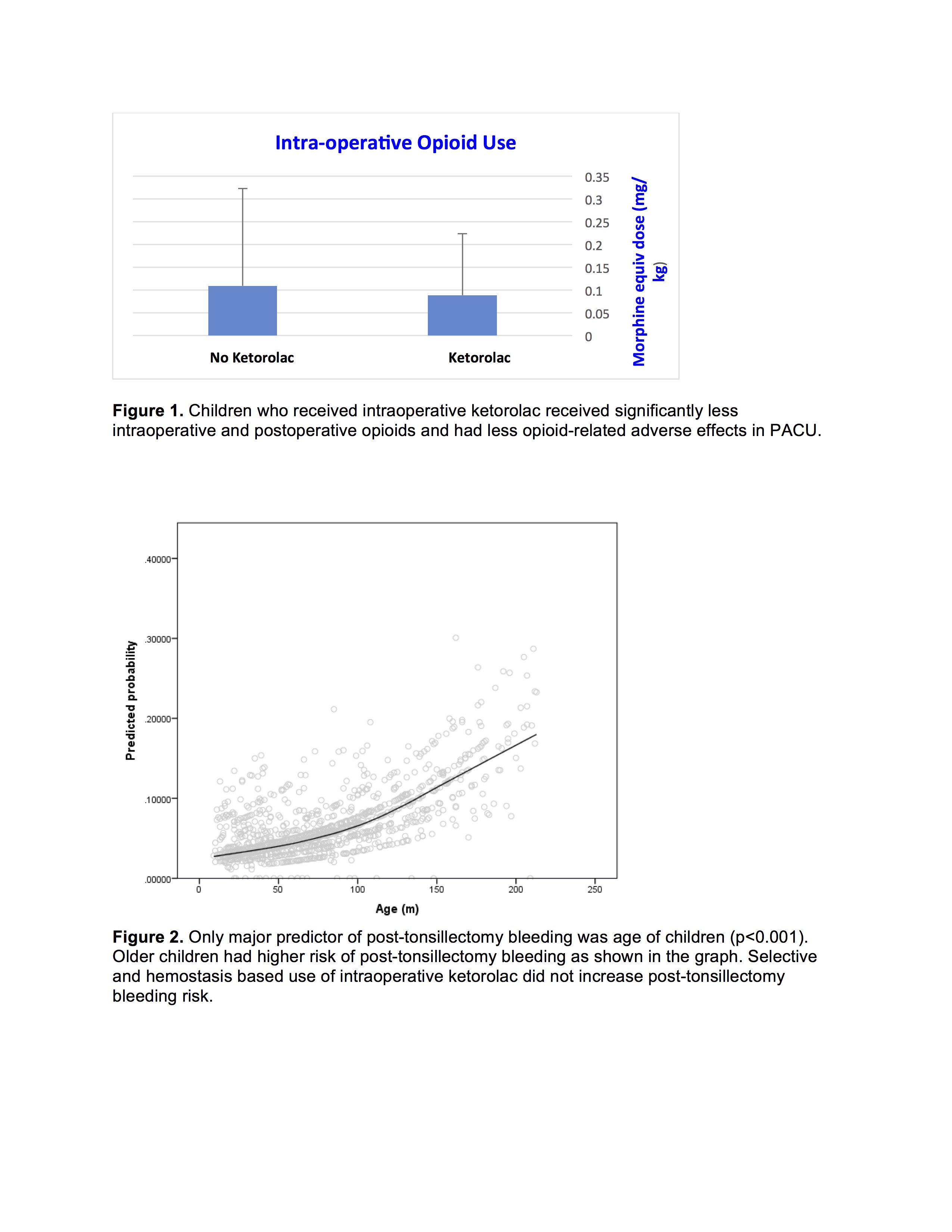
Results: Between 2013 and 2017, 1322 children who had tonsillectomy were included in the study. There were 733 boys and 589 girls with an average age of 6.2 ± 3.8 years. Patients were divided among those who received (K/+, N=669) and did not receive (K/-, N=653) intra-operative intravenous ketorolac. Between the two groups, no statistical difference was found in: post-operative hemorrhage (K/+ 5.7% v K/- 6.9%, RR 0.82, P=0.37); operative intervention for hemostasis (K/+ 62.1% v K/- 58.7%, RR 1.06, P=0.75); and time to hemorrhage (K/- 5.6 v K/+ 6.2 d., p=0.55). Age of the child was significantly predictive of post-operative hemorrhage (p<0.001). K/+ patients received less intra-operative opioids (K/+ 0.089 v K/- 0.11 mg/kg, p<0.05). K/+ patients had less post-operative opioid doses (K/+ 1.59 v K/- 1.86, p<0.05) and overall dose (0.035 v 0.041 mg/kg, p<0.05).
Conclusions: Intra-operative, intravenous administration of ketorolac after satisfactory hemostasis following tonsillectomy did not increase risk of post-operative hemorrhage. By timing administration of intra-operative ketorolac after satisfactory hemostasis, we demonstrated no higher risk of post-tonsillectomy bleeding while providing opioid-sparing analgesic benefits. Surgical-decision based timing of intraoperative ketorolac after satisfactory hemostasis may be a better analgesic strategy than avoiding intraoperative ketorolac all together or giving intraoperative ketorolac for all children undergoing tonsillectomy.
-
 NM-221 Image 1
NM-221 Image 1
Top










