
NM-226
Anomalous Left Coronary Artery from the Pulmonary Artery in an Asymptomatic Two year old after Patent Ductus Arteriosus Closure: A Near Miss Case Report
Alcos S, Zabala L, Arar Y, Dimas V
University of Texas - Southwestern, Dallas, TX, USA
Anomalous Left Coronary Artery from the Pulmonary Artery (ALCAPA) accounts for less than 0.5% of congenital heart anomalies (1). ALCAPA usually results in congestive heart failure with left ventricular dysfunction early in life, but may be asymptomatic if a patent ductus arteriosus (PDA) is present. In this case report, we present a patient who had a PDA with ALCAPA likely resulting in delayed diagnosis secondary to maintained perfusion in the anomalous coronary.
A 2/6 continuous heart murmur was heard at 2 years of age in our previously healthy patient. An echocardiogram showed a moderate PDA, trivial mitral regurgitation, and dilated left ventricle with normal systolic function. She underwent successful transcatheter device closure of her PDA. Her coronary anomaly was not detected during the catheterization.
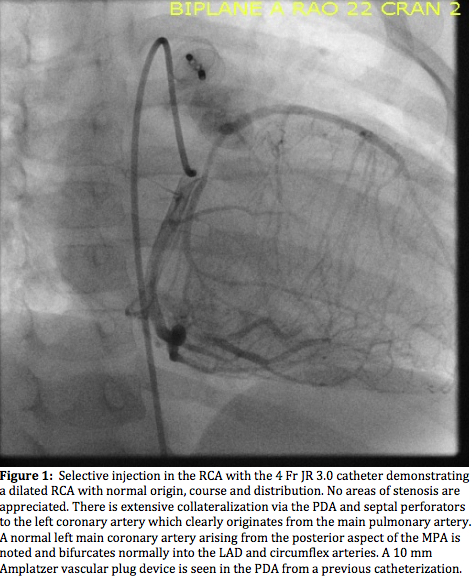
At her follow up visit, her echocardiogram had similar findings; however echobright mitral valve papillary muscles and a coronary artery fistula to the main pulmonary artery were noted. The patient returned to the catheterization lab for a planned occlusion of the coronary artery fistula. Aortic root angiography demonstrated a single, dilated right coronary artery. Selective injection confirmed the diagnosis of ALCAPA. The next day, the patient underwent successful ALCAPA repair by implantation of the left coronary artery into the aorta. The patient’s recovery period was uneventful.
In ALCAPA, prenatally through the first weeks of life, the persistently elevated PVR allows for adequate antegrade perfusion to the anomalous coronary. As PVR drops, coronary steal to the pulmonary circulation occurs, resulting in ischemia. The presence of a moderate PDA likely maintained adequately elevated pulmonary pressures to allow for antegrade flow through the left coronary artery.
Currently there are no reported cases of ALCAPA status post PDA device closure who had successful surgical repair to our knowledge. Once closure of the PDA was performed, the pulmonary artery pressures likely lowered resulting in worsening ischemia. This was seen on echocardiogram in the form of echobright papillary muscles. By angiogram, the patient’s coronary artery system was well collateralized consistent with chronic ischemia.
ALCAPA is an important diagnosis to make prior to any intervention. The anesthesiologist must adapt his/her anesthetic management with this finding. Measures to mildly increase PVR (i.e. mild hypercapnia, low fiO2) can help minimize the coronary steal phenomenon and prevent further myocardial damage (2). This case reminds us how important it is to systematically evaluate all patients with congenital heart disease on every encounter. Prior knowledge of compromised coronary flow would be essential to enable the appropriate anesthetic management, and avoid potentially life threatening complications.
1) Korkmaz et al. Iran J Radiol. 2017
2) Andropoulos et al. Anesthesia for Congenital Heart Disease, 2nd ed., 2010
-
 NM-226 Image 1
NM-226 Image 1
Top










